Chronic Pain
Chronic pelvic pain
Management by Charbel Kortbawi, osteopath in Paris 16, at the Cabinet Victor Hugo — 7 rue Georges Ville (75016).
Chronic pelvic pain: definition, causes and management
Definition of chronic pelvic pain
Chronic pelvic pain (CPP) is a complex, persistent and often disabling condition that affects many women and men worldwide. It is characterised by pain located in the pelvic region, lasting for more than six months, and is associated with a significant impairment of patients' quality of life.
Symptoms of CPP
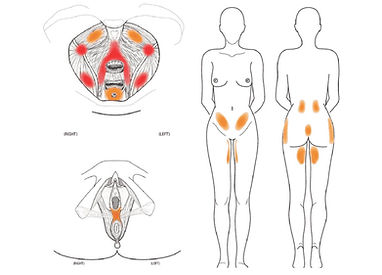
CPP is defined as non-cyclical pain in the pelvic region, persistent or recurrent, which cannot be fully explained by specific pathological causes such as an acute infection or cancer. It may be accompanied by urinary, digestive, sexual and musculoskeletal symptoms: lower abdominal pain, discomfort during sexual intercourse (dyspareunia), pain on urination or defaecation, and increased sensitivity in the pelvic region.

Risk factors for chronic pelvic pain
Risk factors increase when the patient:
- has a history of pelvic inflammatory disease
- has experienced a difficult pregnancy or delivery
- has undergone abdominal surgery or radiotherapy
- suffers from infertility problems
- has a history of physical or sexual abuse
Pathophysiology
The pathophysiology of CPP is complex and involves several mechanisms, including neuromuscular dysfunction, abnormalities of pain perception and psycho-emotional disorders. One of the central mechanisms is central sensitisation, a phenomenon in which the central nervous system amplifies pain signals, making non-painful stimuli painful. People with CPP may also suffer from pelvic muscular dysfunctions, visceral adhesions and myofascial restrictions.
Chronic pelvi-perineal pain is the sum of several clinical entities that are expressed to different degrees in each person; hence the value of a comprehensive, multidisciplinary management.
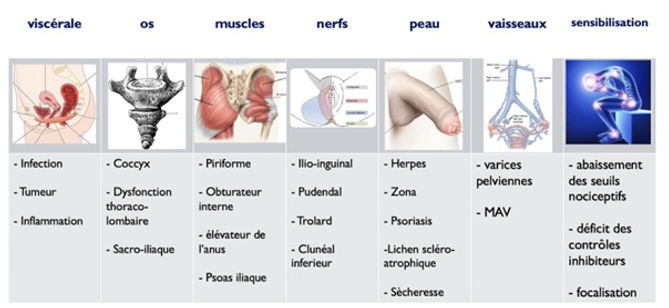
Within CPP, the following components can be distinguished:
- The neuropathic component
- The muscular component
- The osteo-articular component
- The psycho-emotional component
- Central sensitisation of pain
Treatment of chronic pelvic pain
Multidisciplinary approach to management
The management of CPP is multidisciplinary, including pharmacological treatments (analgesics, anti-inflammatories, muscle relaxants, antidepressants), psychological interventions (cognitive behavioural therapy), therapeutic patient education, and sometimes surgical interventions, in particular if mechanical causes such as endometriosis are identified.
Osteopathy and manual therapy in chronic pelvic pain
Treatment by osteopathy will have an effect on the myofascial and articular component of chronic pelvic pain.
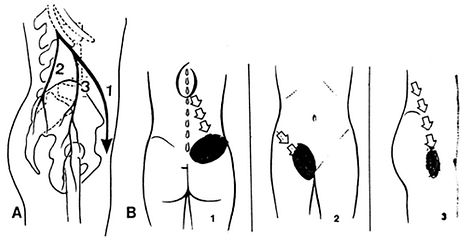
Myofascial dysfunction of the pelvic floor is a source of pain frequently observed in women with chronic pelvic pain. Abdominal myofascial pain, pelvic girdle pain, low back pain, referred hip pain, joint hypermobility and postural imbalances can contribute to chronic pelvic pain.
Osteopathy and manual therapy are approaches increasingly recognised for the management of CPP, with studies showing a significant reduction in pain and an improvement in patients' quality of life. Osteopathic techniques include gentle and specific manipulations of the muscles, ligaments and organs of the pelvis, aimed at restoring mobility and reducing tension in the pelvic region.
Manual therapies, such as myofascial release, target the restrictions at muscular level which, in case of persistent tension, can intensify pelvic pain. These techniques also promote better blood circulation and reduce inflammation.
Frequently Asked Questions
FAQ
How does osteopathy treat chronic pelvic pain?
Osteopathy works on the tension of the pelvic floor muscles, restrictions in the mobility of the sacrum, hips and coccyx, as well as on visceral dysfunctions. The techniques used are gentle and adapted, without forced manipulation of the painful area.
Can chronic pelvic pain be linked to endometriosis?
Yes, endometriosis is a frequent cause of chronic pelvic pain. Osteopathy does not treat endometriosis itself, but can significantly reduce the associated pain by acting on tissue adhesions, muscular tension and articular restrictions of the pelvis.
How many sessions to relieve chronic pelvic pain?
The number of sessions varies depending on the origin of the pain. On average, 4 to 8 sessions are needed, spaced 3 to 6 weeks apart. For complex causes such as endometriosis or levator ani syndrome, follow-up over 6 to 12 months is recommended.
Can a man suffer from chronic pelvic pain and consult an osteopath?
Absolutely. Chronic pelvic pain in men (chronic prostatitis, levator ani syndrome, perineal pain) is frequently under-diagnosed. Osteopathy provides significant help by treating pelvic floor tension and sacroiliac dysfunctions.