Sports Osteopathy — Paris 16
Shin splints in athletes
Care by Charbel Kortbawi, osteopath in Paris 16, at the Victor Hugo practice — 7 rue Georges Ville (75016).
Medial tibial stress syndrome (MTSS): causes, diagnosis, conservative treatment and prevention.
Management of shin splints
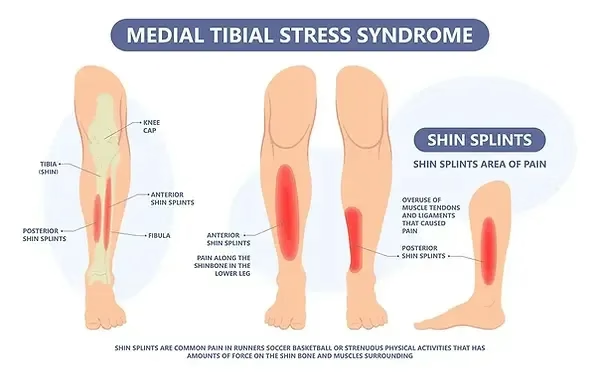
What are shin splints?
Periostitis is an inflammation of the periosteum, the fibrous membrane covering the bones. Shin splints, also known as medial tibial stress syndrome (MTSS), is an overuse injury of the periosteum, frequent in athletes, particularly in runners. It manifests as diffuse pain along the inner border of the tibia, caused by repeated microtraumas. Although benign in most cases, a lack of appropriate treatment can lead to complications such as stress fractures.
Causes of shin splints
Shin splints result from chronic mechanical overload of the tibia, exceeding the natural bone repair capacity. The muscles surrounding the tibia (such as tibialis anterior, tibialis posterior and soleus) play a crucial role in the onset of this pathology. In the event of muscular dysfunction, the stresses on the bone increase, favouring the onset of periosteal inflammation, bone microfractures and, potentially, stress fractures.
Establishing a diagnosis of shin splints
Symptoms
- Diffuse and localised pain on the medial border of the tibia.
- Pain that is worse at the start of exercise, sometimes attenuated after warm-up but may persist at rest.
Risk factors
- Sudden changes in the intensity or duration of training.
- Running on hard or uneven surfaces.
- Biomechanical abnormalities: hyperpronation and flattening of the foot arch, muscular imbalances, leg length differences.
- Affects women more than men.
Clinical examination and imaging
- Tenderness on palpation of the tibial border.
- X-ray to rule out a stress fracture.
- MRI for early detection of bone and periosteal lesions.

Management and treatment of shin splints in athletes
Acute phase
- Relative rest: reduce or stop aggravating activities (2 to 6 weeks).
- Cryotherapy: apply ice for 15 to 20 minutes after effort.
- Analgesics/NSAIDs: to limit pain and inflammation.
Subacute phase
- Adaptation of training: favour low-impact activities (cycling, swimming).
- Muscle strengthening and stretching: stretching of the calf muscles (triceps surae), strengthening of the stabilising muscles (foot, trunk, hips).
- Manual therapy and osteopathy to eliminate adaptations and joint and muscular stiffness.
- Appropriate footwear and, if needed, insoles to correct biomechanical abnormalities.
Complementary approaches
- Extracorporeal shock wave therapy (ESWT): effective in certain refractory cases.
- Injections: platelet-rich plasma (PRP).
- Acupuncture: possible benefits, although the evidence remains limited.
- Surgery: a rare option, reserved for refractory cases. Results are variable.
Prevention and advice for patients
- Training management: progressively increase the intensity and duration of efforts.
- Strengthening and stretching programme: particularly of the muscles of the lower body.
- Adequate equipment: cushioned shoes to be replaced regularly (every 500 km).
- Biomechanical correction: identify and correct imbalances during a thorough clinical evaluation.
Shin splints are a common but largely avoidable pathology. They are often associated with plantar fasciitis or lower-limb tendinopathy, and may be prevented through simple adjustments. Early and individualised management is essential to prevent progression to stress fractures.
Frequently Asked Questions
How long does it take to recover from shin splints?
The acute phase requires 2 to 6 weeks of relative rest. The gradual return to running may begin once pain at rest has resolved. A complete rehabilitation protocol generally lasts 8 to 12 weeks. Without appropriate management, shin splints may progress to a stress fracture.
Can you run with shin splints?
No, not during the acute phase. It is recommended to stop or significantly reduce running to avoid any progression towards a stress fracture. Low-impact activities (cycling, swimming, aqua jogging) can be practised during convalescence.
What signs distinguish shin splints from a stress fracture?
Shin splints cause diffuse pain along the medial border of the tibia. A stress fracture presents with more localised pain, often more intense and persistent at rest. An MRI is recommended to differentiate the two pathologies.
Can osteopathy treat shin splints?
Yes. Osteopathy addresses the muscular and joint imbalances that overload the tibia, particularly at the foot, ankle and knee. It is indicated in the subacute phase, in addition to rest and strengthening exercises.
How do I prevent shin splints in runners?
Increase training load progressively (the 10% rule), wear appropriate footwear renewed every 500 km, strengthen the stabilising muscles of the foot and trunk, and correct biomechanical abnormalities identified during a clinical assessment.
Related articles