Bruxism: causes, symptoms and treatment
Many patients seek consultation for jaw pain, morning headaches or muscular fatigue on waking — without knowing that bruxism is often the underlying cause. This article presents the current state of knowledge on this complex motor behaviour, as well as the validated approaches to reduce its effects.
Definition and classification
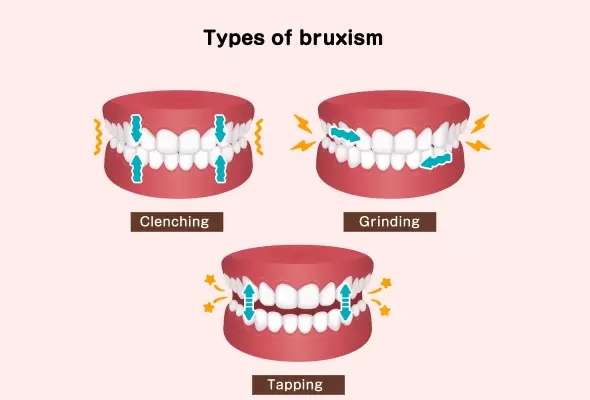
Bruxism is a repetitive activity of the masticatory muscles characterised by clenching or grinding of the teeth and/or by movements of the mandible (bracing or thrusting). Two forms of bruxism are distinguished:
- Sleep bruxism: Sleep bruxism is an activity of the masticatory muscles occurring during sleep. It may be rhythmic (phasic) or non-rhythmic (tonic). In healthy individuals, it is neither a movement disorder nor a sleep disorder.
- Awake bruxism: Awake bruxism is an activity of the masticatory muscles occurring during wakefulness. It is characterised by repetitive or sustained tooth contact and/or by bracing or thrusting of the mandible.
Epidemiology
The prevalence of bruxism varies depending on the diagnostic methods used. A recent meta-analysis by Zieliński et al. (2024) reports the following estimates:
- Overall prevalence of bruxism: approximately 22%
- Sleep bruxism: approximately 21%
- Awake bruxism: approximately 23%
The authors highlight considerable variability between populations studied, a significant influence of diagnostic methods and substantial methodological heterogeneity between studies.
Pathophysiology and causes of bruxism
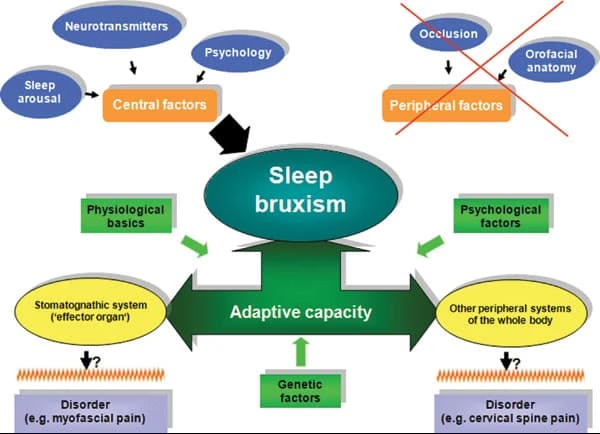
Bruxism is regarded as a behaviour of multifactorial origin, involving central, psychosocial and peripheral factors.
Neurophysiological factors (central nervous system)
Current data indicate that central mechanisms play a predominant role in bruxism, particularly in sleep bruxism. Sleep bruxism occurs preferentially during micro-arousals (the "arousal response"), which correspond to transient activations of the nervous system. These episodes are accompanied by characteristic physiological changes: increased heart rate, respiratory changes, and increased muscular activity.
In this context, the association between bruxism and micro-arousals suggests the involvement of the basal ganglia, brain structures implicated in the regulation and coordination of movement. Several studies suggest this system may be involved via dopaminergic neurotransmitters. This hypothesis is supported by pharmacological observations showing that certain substances influencing dopaminergic neurotransmission modify bruxism activity (L-dopa, amphetamines, SSRIs).
Psychosocial factors
Associations have been observed between bruxism and stress, anxiety and depression.
Peripheral (occlusal) factors
Historically considered determinant, occlusal factors are today only weakly associated with bruxism in adults and are not considered a primary cause.
Central sensitisation
In some patients, repeated muscular contractions may contribute to a sensitisation of nociceptive structures, participating in the chronification of pain.
Diagnosis
The diagnosis of bruxism relies on a grading system proposed by an international consensus, allowing the level of diagnostic certainty to be estimated:
- Possible bruxism: Based solely on the patient's self-report (interview or questionnaires).
- Probable bruxism: Based on the combination of a positive self-report and compatible clinical signs: hypertrophy of the masseter muscles, tooth wear (attrition), tongue indentations, buccal linea alba, pain or fatigue of the masticatory muscles.
- Definite bruxism: Confirmed by instrumental examinations: polysomnography (the reference for sleep bruxism), electromyography.
In clinical practice, a diagnosis of probable bruxism is the most frequently retained. Bruxism may be associated with tooth wear, pain of the masticatory muscles, temporomandibular disorders, headaches or muscular fatigue. The relationship between bruxism and symptoms remains variable and not systematic — bruxism is a potential risk factor rather than a direct and systematic cause of symptoms.
Management and treatment
Management of bruxism is conservative, reversible and multimodal:
Occlusal splint
The occlusal splint is the reference treatment in dental medicine. It protects the dental surfaces and reduces the mechanical loads exerted on the oro-facial structures. However, it does not reliably reduce bruxism activity.
Manual therapy and osteopathy
Manual therapies can contribute to improving pain and mandibular function. The level of evidence is moderate. They should be integrated within a comprehensive management approach.
Cognitive behavioural therapy (CBT)
CBT acts on psychosocial factors, particularly stress and parafunctional behaviours. It has a high level of evidence in the management of chronic pain and temporomandibular disorders.
Biofeedback
Biofeedback is particularly indicated for awake bruxism. It allows the patient to become aware of their muscular activity and improve its control.
Botulinum toxin
Botulinum toxin injections may be offered in severe forms resistant to conservative treatments. They reduce the force of muscular contraction and decrease pain. Their effect is temporary (3 to 6 months).
Stress management
Relaxation techniques, breathing exercises, meditation and improving sleep hygiene.
Specialist osteopathy for bruxism in Paris 16
As an osteopath specialising in pain management and neuroscience, the management of bruxism forms part of a comprehensive, patient-centred approach. The objective is not solely to treat muscular tensions, but to understand the underlying mechanisms involving the nervous system, stress and behavioural habits.
Management includes in particular:
- a precise evaluation of pain and associated disorders (jaw, neck, headaches)
- targeted manual techniques aimed at improving the function of the masticatory muscles and associated structures
- therapeutic education, enabling the patient to better understand their bruxism and identify triggering factors
- nervous-system regulation strategies (breathing, relaxation, awareness of tensions)
- personalised advice adapted to the patient's lifestyle and constraints
Conclusion
Bruxism is a complex, multifactorial motor behaviour, primarily regulated by central mechanisms. Its management relies on an individualised approach aimed at reducing its clinical consequences and acting on risk factors. A multimodal strategy integrating dental, behavioural and musculoskeletal approaches appears the most coherent in light of current scientific data.
References
- Lobbezoo F, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013;40(1):2–4.
- Lobbezoo F, et al. International consensus on the assessment of bruxism. J Oral Rehabil. 2018;45(11):837–844.
- Zieliński G, et al. Global prevalence of sleep bruxism and awake bruxism. J Clin Med. 2024;13(14):4259.
- Lavigne GJ, et al. Neurobiological mechanisms involved in sleep bruxism. Crit Rev Oral Biol Med. 2003;14(1):30–46.
- Lal SJ, et al. Bruxism Management. StatPearls. 2024.
- Riley P, et al. Oral splints for TMD or bruxism: a systematic review. Br Dent J. 2020;228:191–197.
- Amorim CSM, et al. Effect of physical therapy in bruxism treatment: a systematic review. J Manipulative Physiol Ther. 2018;41(5):389–404.
Frequently asked questions (FAQ)
Can osteopathy treat bruxism?
Osteopathy relieves the muscular tensions linked to bruxism (masseters, temporalis, pterygoids) and reduces the frequency of episodes. It does not address the psychological component of bruxism, for which CBT or stress management is recommended.
Should I see a dentist or an osteopath for bruxism?
The two approaches are complementary. The dentist provides an occlusal splint to protect the teeth. The osteopath works on the muscular and articular tensions of the jaw (TMJ) to reduce pain and improve mobility.
What are the symptoms of bruxism?
Bruxism presents as jaw pain on waking, morning headaches, tooth wear, TMJ clicking and sometimes neck pain. These symptoms often worsen during periods of stress.
How many osteopathy sessions are needed for bruxism?
Generally, 3 to 5 sessions are sufficient to significantly reduce the muscular tensions linked to bruxism. Regular follow-up may be useful, particularly during periods of intense stress.