Myofascial trigger points: mechanisms, diagnosis and treatment
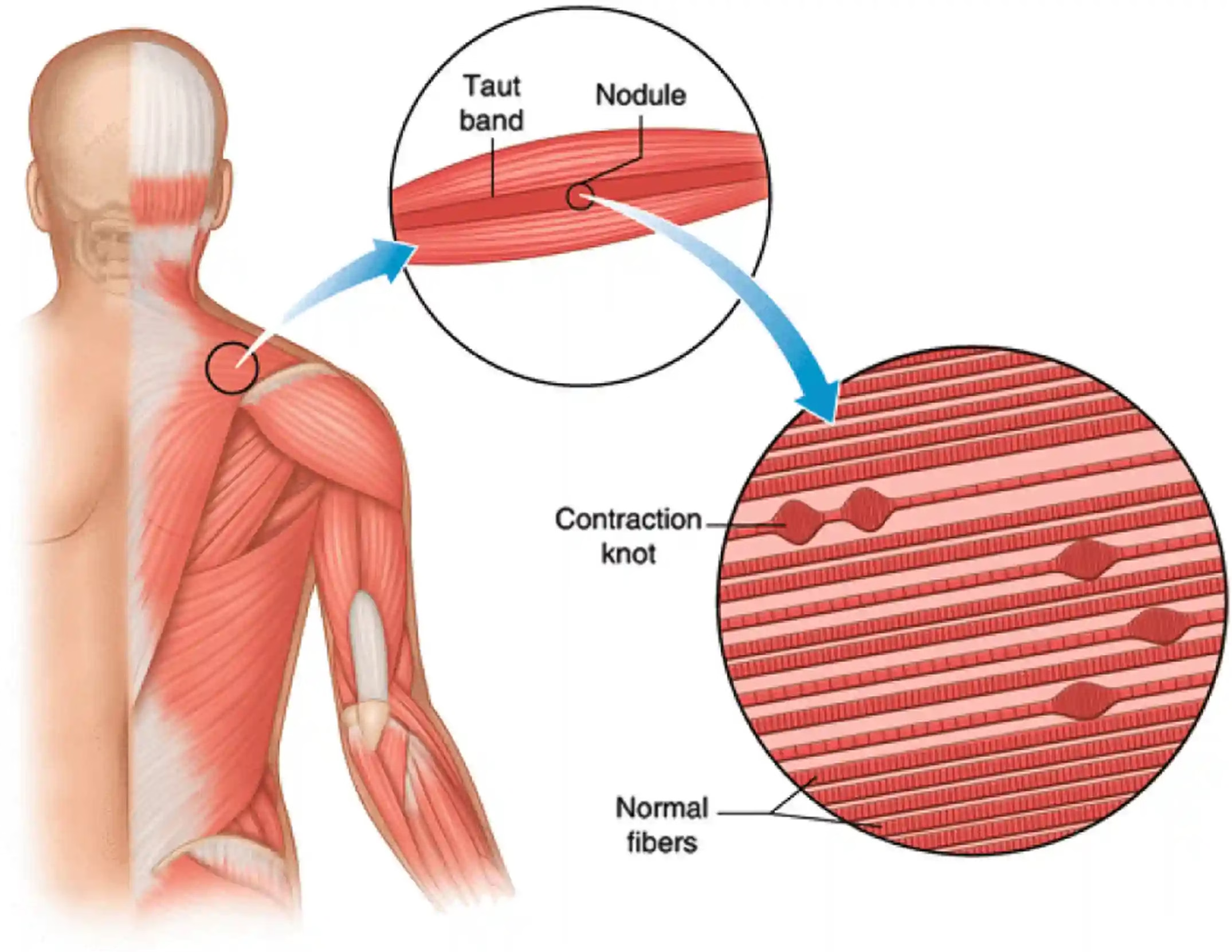
What is a myofascial trigger point? Myofascial trigger points (MTrPs) are hypersensitive areas located within a taut band of skeletal muscle. Palpable as painful nodules, these points are responsible for local or referred pain, muscular stiffness and sometimes an alteration of neuromuscular function. Their clinical description and precise mapping were systematised by Dr Janet Travell from the 1940s onwards, then developed further and widely disseminated in collaboration with Dr David Simons in the 1980s. Their work laid the foundations of the modern concept of myofascial pain, now integrated into the management of musculoskeletal pain.
How to recognise a trigger point.
- Presence of a hypersensitive nodule within a contracted muscular cord.
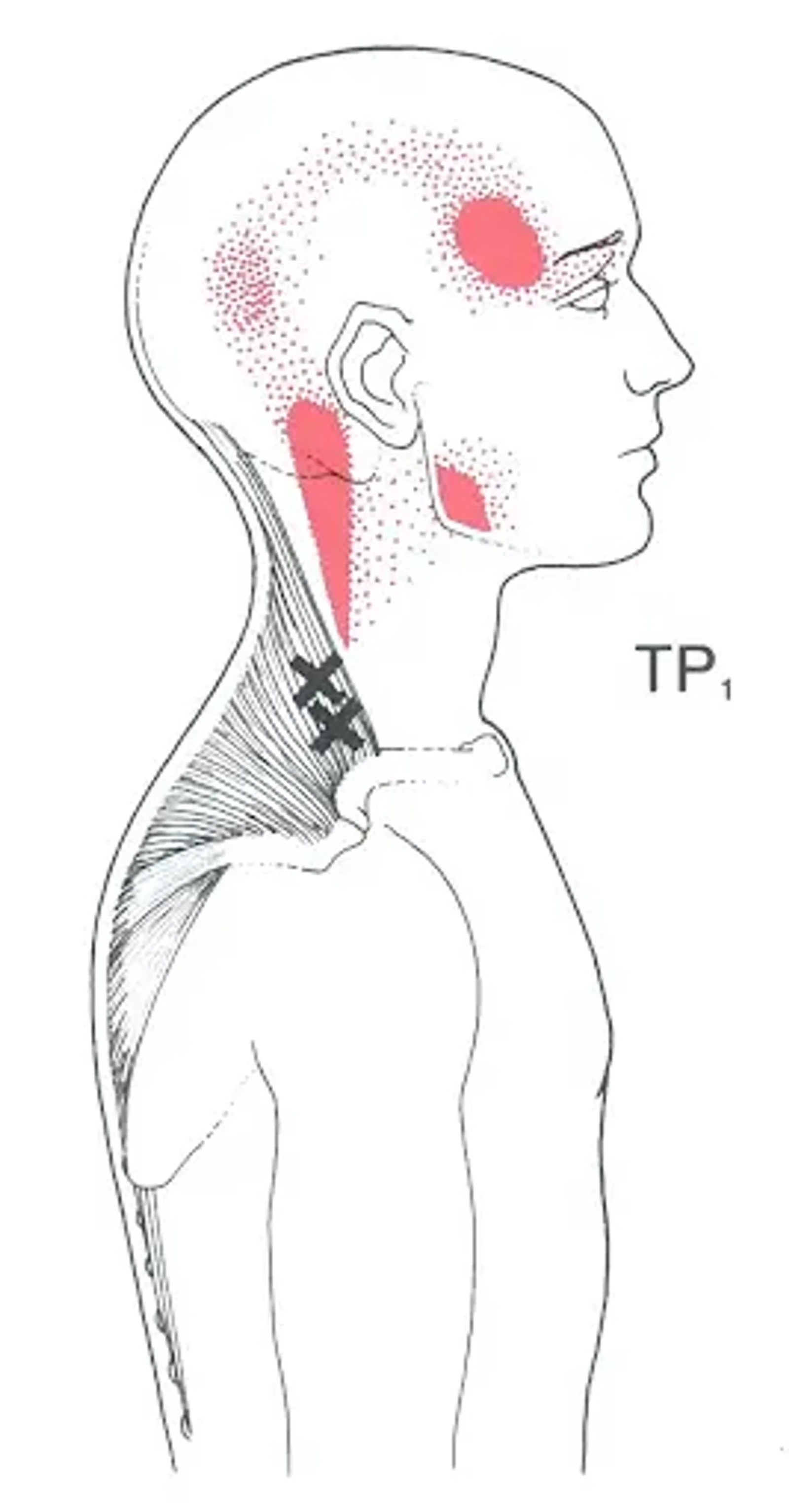
- Referred pain at a distance when pressure is applied to this nodule.
- Appearance of a brief, local muscular contraction (twitch) upon stimulation.
- Exaggerated painful reaction to moderate pressure (hypersensitivity).
Two types of trigger points are distinguished:
- Active: generates spontaneous pain and reproduces the patient's symptoms.
- Latent: silent at rest but painful under pressure or during movement.
Causes of trigger points.
MTrPs are linked to a disturbance of the neuromuscular junction. Excessive release of acetylcholine triggers a local contraction, reducing blood flow and causing an accumulation of pro-inflammatory substances. This results in hypersensitisation of peripheral pain receptors and possibly central sensitisation in case of prolonged pain.
Common causes of trigger points
- Muscular overload or overuse (repeated exertion, prolonged poor posture).
- Direct trauma (impact, contusion).
- Prolonged immobilisation or inactivity.
- Emotional stress.
- Biomechanical imbalances (feet, pelvis, spine).
Symptoms of trigger points.
Symptoms can be varied and often misleading:
- Local or referred muscular pain.
- Reduced joint range of motion.
- Muscular weakness.
- Tingling sensations without neurological involvement.
Conditions associated with trigger points.
Myofascial trigger points are frequently implicated in many musculoskeletal disorders and chronic pain conditions. They do not constitute a pathology in themselves, but can sustain, amplify or mimic various conditions. They are found in particular in the following contexts:
- Fibromyalgia: although of complex aetiology, this diffuse pain syndrome is often associated with the presence of multiple active trigger points, contributing to chronic pain.
- Chronic myofascial syndrome: a distinct clinical entity, characterised by the persistence of active MTrPs responsible for regional pain, often poorly localised and resistant to conventional treatments.
- Central sensitisation syndromes: in some chronic pain conditions with no organic visible cause, trigger points can sustain hyperexcitability of the central nervous system, as in tension headaches, jaw pain, low back pain, etc.
- Functional disorders linked to posture and repetitive movement: biomechanical imbalances, prolonged positions or repeated efforts favour the appearance of trigger points, notably in the muscles of the back or neck.
Identification and management of MTrPs in these contexts often reduces pain intensity, restores mobility and limits the chronification of symptoms.
Treatment of myofascial trigger points
The management of trigger points relies on a multimodal approach combining manual therapies, specific techniques, therapeutic exercises and rehabilitation. The aim is to deactivate the painful points, restore muscular function and correct the factors of recurrence.
Manual therapy and osteopathy.
- Sustained ischaemic pressure: application of progressive pressure on the painful point until reduction of sensitivity.
- Post-isometric stretch: passive mobilisation of the muscle after a gentle isometric contraction, to release tension.
- Myofascial release techniques: deep work on the soft tissues to free fascial adhesions.
- Deep transverse massage: to disorganise contracted fibres and stimulate local circulation. Treatment of trigger points by ischaemic pressure.
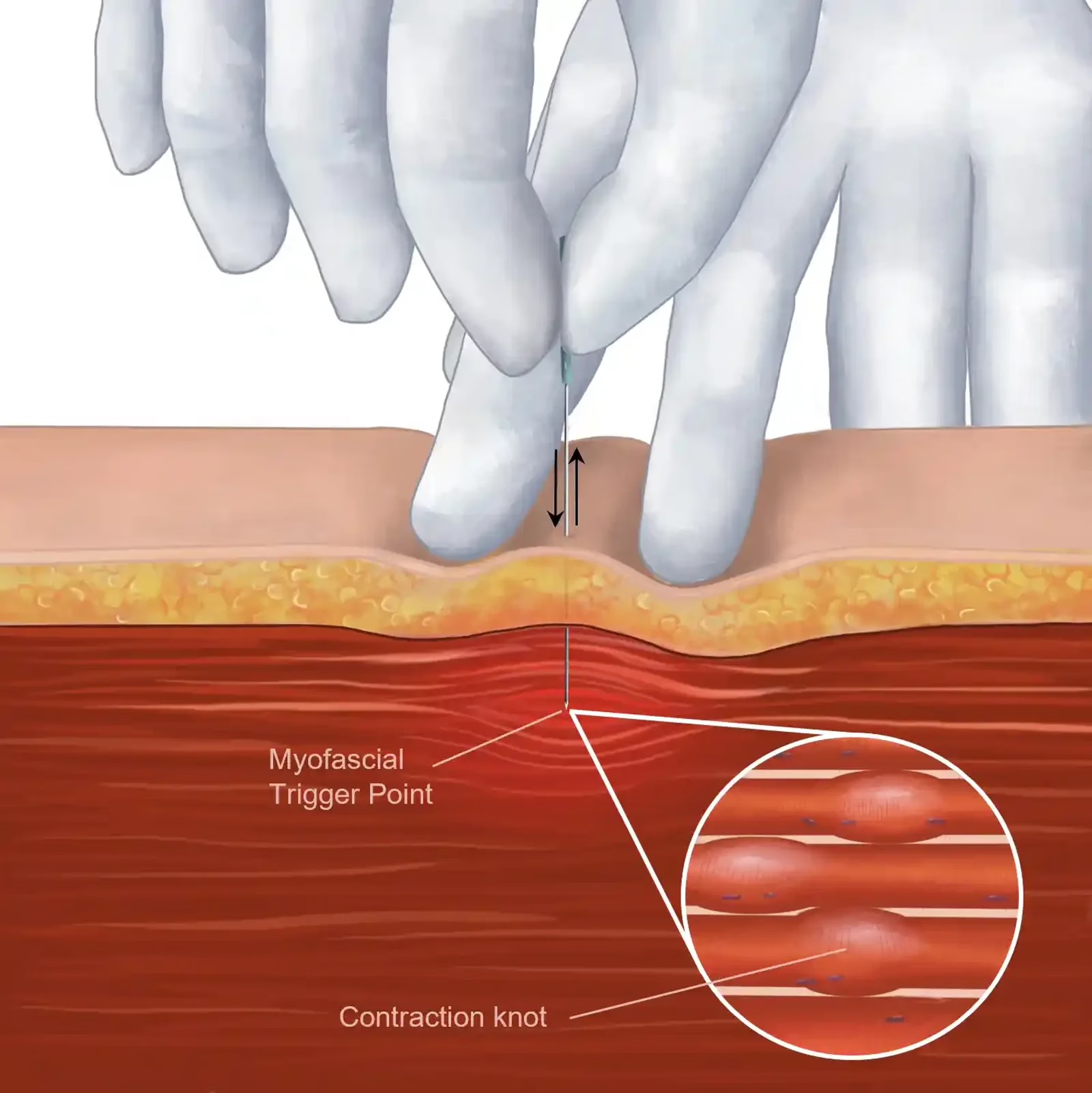

Dry needling.
Physical exercise.
- Targeted active stretches: to restore muscle length and prevent reactivation of MTrPs.
- Progressive muscle strengthening: essential to rebalance muscle chains and avoid overload.
- Postural retraining: to correct postural or movement habits favouring the appearance of trigger points.
Spray and stretch technique.
This technique consists of applying a cooling spray on the skin above the muscle concerned, followed immediately by a passive stretch. It is used to inhibit nociceptive reflex arcs and facilitate muscle lengthening.
Local anaesthetic injections.
In some cases, an intramuscular injection of lidocaine may be given into the trigger point to deactivate its activity. This method is generally reserved for resistant forms and is performed under medical supervision, sometimes as an adjunct to other manual or rehabilitation approaches.
Benefits of osteopathic management
Osteopathic approach to the management of trigger points.
Osteopathy offers comprehensive and personalised management of the patient suffering from trigger points. It is not limited to local treatment, but fits within a global vision of body function and its imbalances.
- Targeted manual therapy.
- Postural rebalancing: correction of asymmetries, imbalances of weight-bearing or joint mobility that sustain chronic tensions.
- Therapeutic education and autonomy: personalised advice, self-stretching exercises, postural hygiene and strategies for self-regulating pain.
Conclusion: a global approach to lasting relief of myofascial pain
Trigger points represent a common but often underestimated cause of chronic muscular pain. Effective management requires a structured, multidisciplinary approach adapted to the specific features of each patient.
Osteopathy positions itself as a comprehensive therapeutic strategy. By restoring the overall balance of the body, supporting the patient in understanding their pain and fostering autonomy, it helps prevent recurrence and lastingly improve quality of life.
Frequently asked questions (FAQ)
What is a myofascial trigger point?
A trigger point is a hypersensitive area localised within a muscle, characterised by a palpable taut band of tissue. Its compression reproduces local pain and often referred pain at a distance, in a typical pattern depending on the muscle concerned.
How does osteopathy treat trigger points?
Osteopathy uses myofascial release techniques, ischaemic compression and stretching of taut bands to deactivate trigger points. These techniques reduce local and referred pain in 2 to 4 sessions in most cases.
Can trigger points cause pain at a distance?
Yes, this is their main characteristic. A trigger point in the trapezius can cause headaches, a point in the psoas can refer to the lower back, and a point in the masseters can cause dental pain. The referred pain map guides diagnosis.
What is the difference between a point gâchette and a trigger point?
They are two terms for the same thing. 'Trigger point' is the English term used by Travell & Simons (1999), translated in French as 'point gâchette'. Myofascial pain syndrome with trigger points is a common and under-diagnosed cause of chronic pain.