Understanding the Impact of Sleep on Chronic Pain
A short, evidence-based overview — every claim sourced to a peer-reviewed PubMed-indexed study.
A two-way street
Pain disturbs sleep, and disturbed sleep makes pain more likely. Across the past decade, large prospective cohorts and experimental studies have shown that the arrow running from poor sleep to future pain is at least as strong as the reverse [1,2]. A 2026 narrative review in EBioMedicine summarizes this evidence across the lifespan: in childhood and adolescence poor sleep may precede the emergence of pain through neurodevelopmental impacts on the way pain — and emotion — are later regulated; in adulthood, sleep interacts with lifestyle, psychological state and occupational stressors; and in older adults, chronic pain and comorbidities such as sleep apnoea and depression further impair sleep, reinforcing a vicious cycle [9].
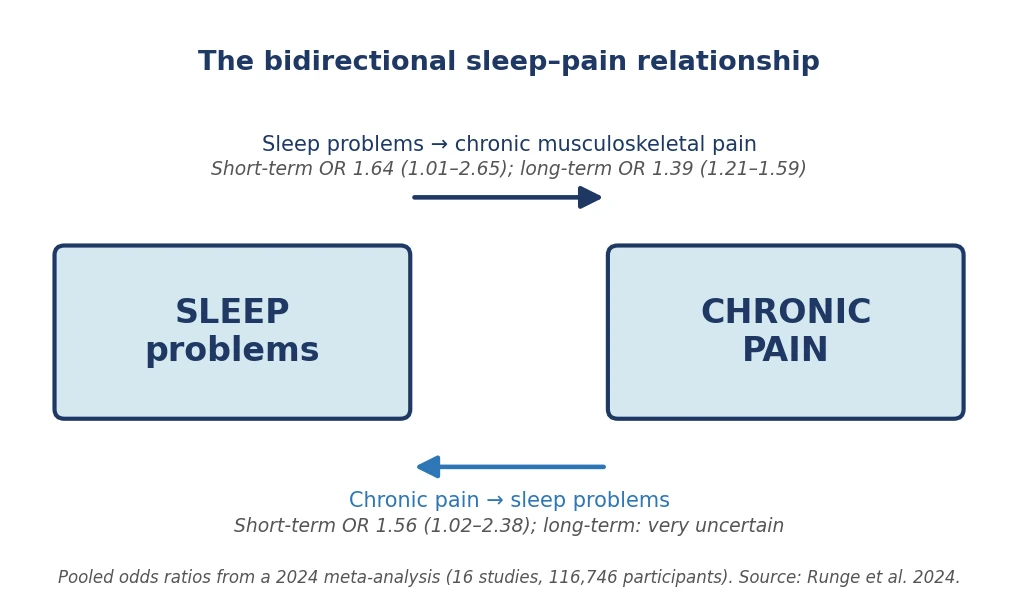
The strongest evidence comes from a large 2024 meta-analysis that pooled sixteen prospective cohort studies and nearly 117,000 participants followed over time. The finding is unambiguous: people with sleep problems at the start of follow-up went on to develop chronic musculoskeletal pain more often than people who slept well — a clear effect over the short term, and one that remained measurable years later. The link also runs the other way, with chronic pain in turn making sleep problems more likely; but the long-term evidence in that direction was judged too uncertain to draw firm conclusions [2].
The Norwegian HUNT study, which followed 13,429 adults with no chronic musculoskeletal pain at baseline for eleven years, points the same way. Among those who had insomnia at baseline, the risk of developing widespread pain — meaning pain felt in several parts of the body — was nearly 60% higher, and almost doubled when the pain extended to five or more body regions [3].
A neurobiological review puts the asymmetry plainly: "emerging evidence suggests that sleep disturbances have a stronger influence on subsequent pain than vice versa" [4].

Sleep loss sensitizes the pain system
In a controlled experiment, 21 healthy adults had their sleep deliberately cut to about half their usual duration for two nights. The result: their pain sensitivity went up. For the most intense electrical stimuli, they reported feeling more pain than before; their brains responded more strongly to those stimuli; and less pressure on the trapezius muscle was needed to reach the pain threshold [5].
Why this happens
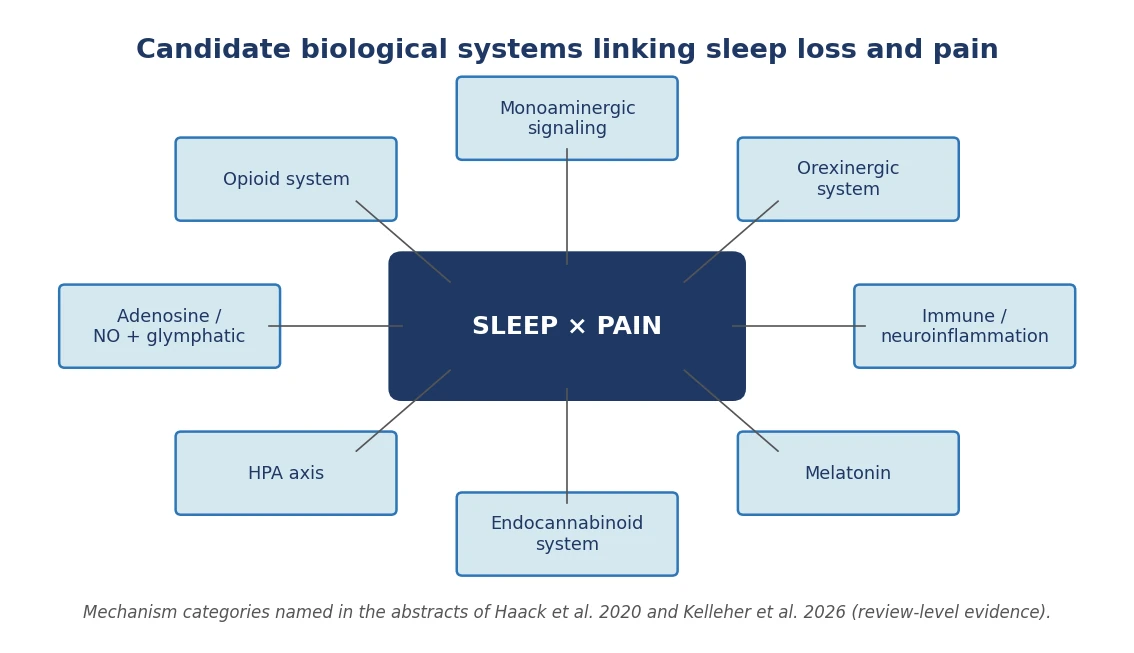
A 2020 review in Neuropsychopharmacology catalogues the biological systems thought to mediate the modulation of pain by sleep deficiency: the opioid, monoaminergic, orexinergic, immune, melatonin, and endocannabinoid systems; the hypothalamus–pituitary–adrenal (HPA) axis; and adenosine and nitric oxide signaling. The same review notes that some commonly used medications can amplify pain by disturbing sleep [1]. The 2026 EBioMedicine review highlights three shared candidate mechanisms operating across the lifespan — HPA-axis dysregulation, neuroinflammation, and impaired glymphatic clearance — and frames early sleep disturbance as a modifiable risk factor for later pain [9].
Which treatments actually help?
Among non-medication options, the treatment with the strongest evidence is cognitive behavioral therapy for insomnia, often abbreviated CBT-I. It is a structured programme delivered by a trained professional, built around well-defined techniques — quite different from the generic "tips for sleeping better" you might read online.
Several studies converge. In 100 adults with both knee osteoarthritis and insomnia, CBT-I reduced nighttime awakenings, and that improvement in sleep predicted a subsequent decrease in pain. Across the trial, about one in three participants saw their pain drop by 30% or more [6]. A large 2022 review pooling sixteen clinical trials reached the same conclusion: CBT-I improves sleep, pain, day-to-day function, and mood. A different form of cognitive behavioural therapy that focused only on pain did not significantly differ from the control condition for these patients [7].
The benefit on pain itself is not, however, universal. A recent trial in 123 adults with both nonspecific chronic spinal pain (neck or back) and insomnia compared standard pain care with or without CBT-I added. After one year, pain had decreased in both groups — somewhat more with CBT-I, but not enough for the difference to be statistically clear. CBT-I did clearly improve sleep, mood, and fatigue, with no serious side effects [8].
The take-home message: improving sleep helps, sometimes considerably — but it does not mechanically "cure" chronic pain.
In practice: what works, what doesn't
What can you actually do when bad sleep and chronic pain travel together? The largest analysis to date — pooling more than 240 clinical trials and over 31,000 patients, published in 2024 in JAMA Psychiatry — gives precise answers, and some of them are surprising [10].
What genuinely helps, when delivered as part of a structured programme with a trained therapist:
- Working on the thoughts and beliefs that keep insomnia going — identifying, challenging, and changing unhelpful beliefs about sleep. This is called cognitive restructuring.
- Mindfulness and Acceptance and Commitment Therapy (ACT). Mindfulness is a meditation practice that develops non-judgmental awareness of one's thoughts, emotions and sensations in the present moment; ACT helps accept the thoughts and feelings linked to insomnia while continuing to act in line with one's own values.
- First limiting time in bed to the average sleep duration plus about 30 minutes, then adjusting it — up or down — depending on how efficient sleep becomes. This is sleep restriction.
- Reconnecting the bed with sleep: getting up at the same time every morning, avoiding daytime naps, only going to bed when sleepy, getting out of bed if unable to sleep, and reserving the bed and bedroom for sleep and intimacy only — known as stimulus control.
What helps less than commonly assumed:
- Generic "sleep hygiene" advice — warm bath, no coffee, no screens at night, and so on. On its own, this has not been shown to reliably restore good sleep.
- Relaxation exercises alone: the same analysis even suggests they may be counterproductive. A finding to interpret cautiously, but one that argues against relying on them as a stand-alone fix.
The format that works best is a structured, in-person programme with a trained therapist [10]. Put differently: if sleep problems are entrenched, reading tips online or taking a supplement is unlikely to be enough. Real, focused care — short but well-conducted — is what makes the difference.
Finally, some pain medications can themselves disturb sleep. If you notice this, raise it with your doctor before changing anything on your own [1].
Bottom line
Disturbed sleep is a robust prospective risk factor for chronic pain, controlled sleep restriction sensitizes the pain system within days, and CBT-I reliably improves sleep in people with comorbid pain — with smaller, condition-dependent effects on pain itself. Sleep is a modifiable lever in chronic pain care, but is not a stand-alone cure.
Frequently asked questions (FAQ)
Can poor sleep cause chronic pain?
Large prospective cohorts show that sleep problems significantly raise the risk of developing chronic musculoskeletal pain: pooled odds ratio 1.64 in the short term and 1.39 in the long term (Runge et al. 2024, 116,746 participants). The effect of poor sleep on subsequent pain appears at least as strong as the reverse.
What non-drug treatment works best?
Cognitive behavioral therapy for insomnia (CBT-I) has the strongest evidence base. The most effective components are cognitive restructuring, third-wave components, sleep restriction and stimulus control, delivered in person (Furukawa et al. 2024, 241 trials, 31,452 participants).
Is sleep-hygiene advice enough?
No. Sleep-hygiene education on its own is not associated with higher insomnia remission (iOR 1.01; 95% CI 0.77–1.32). The active components of CBT-I, delivered by a trained therapist, are needed to obtain the best outcomes.
How few nights of poor sleep can amplify pain?
Two nights of 50% sleep restriction are enough to sensitize the pain system in healthy adults: subjective pain ratings, the pain-evoked EEG response and the pressure pain threshold all change significantly (Matre et al. 2015).
References
- Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45(1):205–216. DOI: 10.1038/s41386-019-0439-z. PMID: 31207606.
- Runge N, Ahmed I, Saueressig T, et al. The bidirectional relationship between sleep problems and chronic musculoskeletal pain: a systematic review with meta-analysis. Pain. 2024;165(11):2455–2467. DOI: 10.1097/j.pain.0000000000003279. PMID: 38809241.
- Uhlig BL, Sand T, Nilsen TI, Mork PJ, Hagen K. Insomnia and risk of chronic musculoskeletal complaints: longitudinal data from the HUNT study, Norway. BMC Musculoskeletal Disorders. 2018;19(1):128. DOI: 10.1186/s12891-018-2035-5. PMID: 29699540.
- Christensen J, Noel M, Mychasiuk R. Neurobiological mechanisms underlying the sleep-pain relationship in adolescence: A review. Neuroscience and Biobehavioral Reviews. 2019;96:401–413. DOI: 10.1016/j.neubiorev.2018.11.006. PMID: 30621863.
- Matre D, Hu L, Viken LA, et al. Experimental Sleep Restriction Facilitates Pain and Electrically Induced Cortical Responses. Sleep. 2015;38(10):1607–1617. DOI: 10.5665/sleep.5058. PMID: 26194577.
- Smith MT, Finan PH, Buenaver LF, et al. Cognitive-behavioral therapy for insomnia in knee osteoarthritis: a randomized, double-blind, active placebo-controlled clinical trial. Arthritis & Rheumatology. 2015;67(5):1221–1233. DOI: 10.1002/art.39048. PMID: 25623343.
- Enomoto K, Adachi T, Fujino H, Kugo M, Tatsumi S, Sasaki J. Comparison of the effectiveness of cognitive behavioral therapy for insomnia, cognitive behavioral therapy for pain, and hybrid cognitive behavioral therapy for insomnia and pain in individuals with comorbid insomnia and chronic pain: A systematic review and network meta-analysis. Sleep Medicine Reviews. 2022;66:101693. DOI: 10.1016/j.smrv.2022.101693. PMID: 36410076.
- Malfliet A, De Baets L, Bilterys T, et al. Cognitive Behavioral Therapy for Insomnia in Pain Management for Nonspecific Chronic Spinal Pain: A Randomized Clinical Trial. JAMA Network Open. 2024;7(8):e2425856. DOI: 10.1001/jamanetworkopen.2024.25856. PMID: 39120902.
- Kelleher EM, Wall A, Seymour B, Irani A. Why sleep matters in chronic pain: evidence across the lifespan. EBioMedicine. 2026;125:106158. DOI: 10.1016/j.ebiom.2026.106158. PMID: 41708400.
- Furukawa Y, Sakata M, Yamamoto R, et al. Components and Delivery Formats of Cognitive Behavioral Therapy for Chronic Insomnia in Adults: A Systematic Review and Component Network Meta-Analysis. JAMA Psychiatry. 2024;81(4):357–365. DOI: 10.1001/jamapsychiatry.2023.5060. PMID: 38231522.
Source database: PubMed (U.S. National Library of Medicine). Citations were verified against article metadata retrieved directly from PubMed; claims are restricted to findings explicitly stated in the cited articles' abstracts. Photo: Unsplash (Unsplash License — free for commercial and non-commercial use). Diagram figures were generated from numerical values reported in the cited abstracts.