Sports Osteopathy — Paris 16
Treatment of athletic pubalgia in Paris 16
Care by Charbel Kortbawi, osteopath in Paris 16, at the Victor Hugo practice — 7 rue Georges Ville (75116).
Osteopathic management of athletic pubalgia: classification, risk factors and conservative treatment.
What is pubalgia?
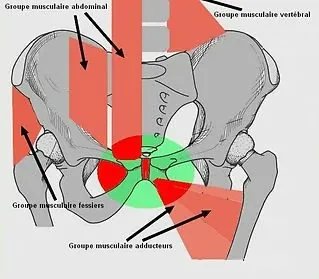
Pubalgia is a complex musculoskeletal pathology that affects the pubic region, an anatomical area grouping together tendinous, articular, muscular, neurological and bony structures. It frequently occurs in athletes practising activities involving rapid changes of direction, sudden accelerations or repetitive movements, such as football, hockey or rugby.
Epidemiology of pubalgia
- Men practising pivoting sports (football, hockey) are twice as much at risk as women.
- Adductor-related pubalgia is the most common form (68%), followed by iliopsoas-related pubalgia (12%).
- Frequent recurrence: a history of pubalgia multiplies the risk of recurrence by 2.4.
Classification and symptoms of pubalgia
The international classification (Doha Agreement meeting — 2015) distinguishes four main types:
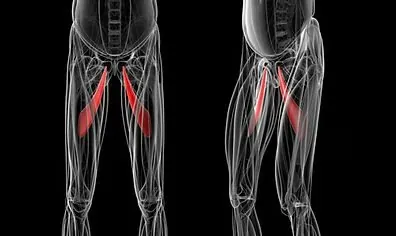
Adductor-related pubalgia
Tendinous or muscular pathologies of the hip adductors. Pain around the proximal insertion of the adductor longus, sometimes radiating towards the medial aspect of the thigh. Pain is often exacerbated by adduction movements or adductor strengthening exercises.
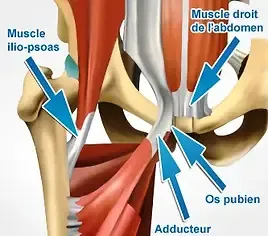
Iliopsoas-related pubalgia
Injury of the iliopsoas tendon or muscle. Pain at the anterior and lateral aspect of the thigh, often felt during resisted hip flexion or stretching of the flexors. Sensation of discomfort in prolonged flexion positions, for example while sitting.
Inguinal forms
Pathologies affecting the inguinal region, including inguinal hernias. Pain localised in the inguinal region, aggravated by physical activity, coughing or contraction of the abdominal muscles. Increased sensitivity on palpation of the lower abdominal wall is frequently observed.
Pubic forms
Injury of the pubic symphysis or surrounding bony structures. Pain localised over the pubic symphysis during movements involving the muscles of the pubic region.
Risk factors of athletic pubalgia
Modifiable intrinsic factors
- Weakness of the hip adductors.
- Imbalance in the adductor/abductor ratio (ideally ≥ 0.9 to prevent pubalgia).
Non-modifiable intrinsic factors
- History of pubalgia.
- Morphological factors (dysplasia, bony asymmetry).
Modifiable extrinsic factors
- Excessive training load.
- Absence of specific exercises for the adductors and hip flexors.
Management and treatment of athletic pubalgia
Conservative treatment
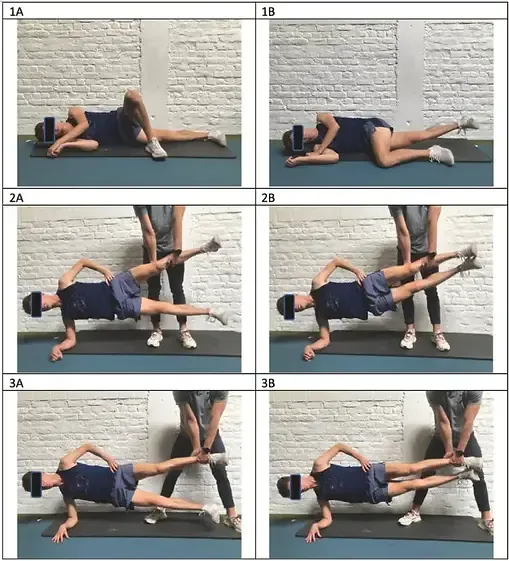
- Targeted active rehabilitation: adductor strengthening (e.g. Copenhagen Adduction Exercise), optimisation of the coordination of interarticular movements to reduce excessive tensions at the pubic region.
- Manual therapy and osteopathy: techniques to improve joint mobility and reduce pain, elimination of postural imbalances and adaptations of the lower limbs, pelvis and spine.
Average duration of return to sport: 12 weeks. An associated tendinopathy may prolong this duration and requires simultaneous management.
Surgical treatment
- Indicated for certain inguinal forms (e.g. hernias or weakness of the abdominal wall).
- Recurrences.
Faster return to sport: 4 to 6 weeks post-intervention.
Prevention
- Specific programmes for adductor strengthening (e.g. Copenhagen Adductor Strengthening Program).
- Monitoring of training load and planning of active rest.
- Biomechanical optimisation through mobility and strengthening exercises.
Frequently Asked Questions
How long does recovery from athletic pubalgia take?
Conservative treatment allows a return to sport on average within 12 weeks. In the case of surgical intervention for an inguinal form, return to sport is faster: 4 to 6 weeks. Active rehabilitation and adductor strengthening are essential to prevent recurrence.
When should I consult an osteopath for athletic pubalgia?
Consult as soon as the first signs appear: groin pain during effort, discomfort during changes of direction, pain on palpation of the pubic symphysis. Early management significantly reduces the risk of chronicity.
What is the difference between athletic pubalgia and an inguinal hernia?
Athletic pubalgia encompasses the tendinous and muscular injuries of the pubic region. An inguinal hernia is a specific form involving weakness of the abdominal wall. These two pathologies may coexist and the Doha 2015 classification distinguishes them clearly.
Which sports carry the highest risk of pubalgia?
Pivoting sports involving rapid changes of direction are the most affected: football (highest risk), ice hockey, rugby, handball. Men are twice as often affected as women.
How do I prevent recurrence of pubalgia?
The Copenhagen Adductor Strengthening programme is the most documented preventive method. It includes specific adductor strengthening exercises, training load monitoring and biomechanical optimisation of the sporting movement.
Related articles