Sports Osteopathy — Paris 16
Tendinopathy treatment
Care provided by Charbel Kortbawi, osteopath in Paris 16, at the Victor Hugo practice — 7 rue Georges Ville (75116).
Pathophysiology, conservative treatment and the contribution of osteopathy and manual therapy in the management of tendinopathies.
Pathophysiology and progression of tendinopathies
Definition: evolution of the term from tendinitis to tendinopathy
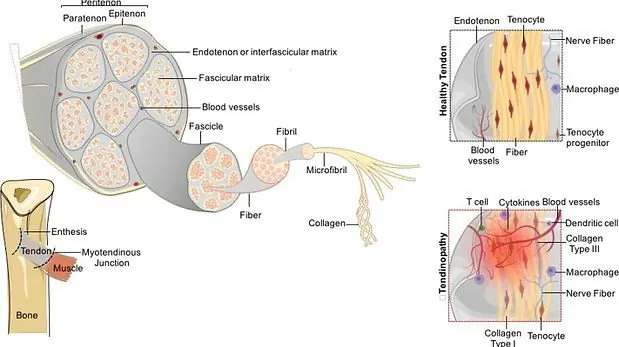
Knowledge about tendinopathies and their management has evolved considerably. The term "tendinitis", which implied an inflammatory reaction as the main mechanism, has today been replaced by "tendinopathy". Current theories suggest that chronic excessive loads or acute stress are responsible for the structural changes observed. These changes can be reversible or progress towards defective healing, then tendon degeneration.
Tendinopathies generally present with a symptomatic triad: pain on stretching, pain during isometric contractions and pain on palpation.
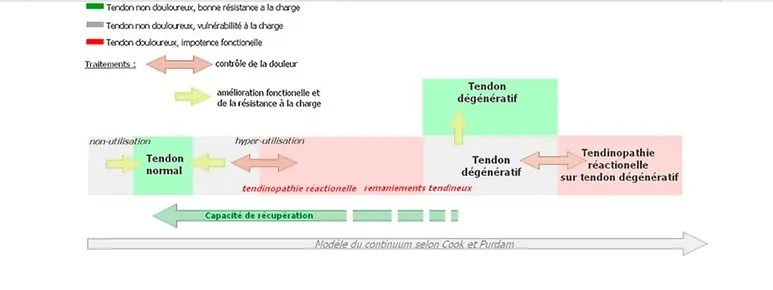
Since 2009, the "tendinopathy continuum" model has become a reference in the literature, dividing the pathology into three successive stages.
Reactive tendinopathy
The first stage of the continuum. It occurs in response to a sudden increase in load on the tendon, for example due to a rapid intensification of training, an unusual activity in a sedentary person, or direct trauma. The cellular reaction is mainly non-inflammatory, but leads to increased production of proteoglycans, which retain water and produce a characteristic ultrasound appearance of tendon thickening. This stage is completely reversible, allowing rapid adaptation to loads.
Tendon disrepair
The second stage involves deeper structural changes, where prolonged overload leads to matrix disorganisation and cell proliferation. This results in localised, heterogeneous thickening visible on ultrasound, with increased vascularisation. Early load management and a suitable rehabilitation programme can help reverse these changes.
Degenerative tendinopathy
The third stage results from chronic overload leading to cellular apoptosis and significant matrix breakdown. The tendon becomes weakened, at risk of rupture, and shows notable vascular and neural proliferation. At this stage, the tendon may require complementary biological treatments such as shock waves or platelet-rich plasma injections to optimise regeneration.
More recently, Cook and Purdam have adjusted their model, showing that tendon lesions are more complex and that a single tendon may simultaneously present reactive and degenerative areas. This observation allows for a personalised therapeutic approach, aiming first to relieve pain and then to strengthen the tendon structure through suitable physical rehabilitation.
Pain management and treatment of tendinopathies
Medical management
Analgesic and anti-inflammatory treatments
Analgesic treatments often provide short- and medium-term clinical improvement. However, administered alone, they show limited long-term benefits, due to the persistence of the altered tendon structure, which leads to a high prevalence of recurrence.
The first-line treatment is to remove the cause of the lesion by resting the tendon and adopting a "wait-and-see" approach. For high-level athletes, it is possible to reduce training intensity without exceeding the pain threshold. Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, are the first-choice treatment in the acute phase.
Corticosteroid injections
Corticosteroid injections, although commonly used, have limited long-term efficacy. The review by Coombs et al. shows that, for lateral epicondylitis, corticosteroids yield inferior outcomes at 26 weeks compared with "wait-and-see" treatment, NSAIDs, manual therapy, or PRP. Corticosteroids also carry risks of side effects: subcutaneous tissue atrophy (9 %), residual pain (8 %), local depigmentation (< 1 %) and, rarely, tendon rupture.
Osteopathic care and rehabilitation
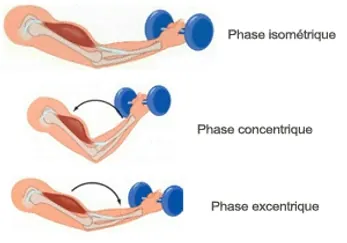
Sustained isometric contraction
Sustained isometric contraction is effective for pain management. The study by Rio et al. in athletes showed that an isometric contraction of the quadriceps (5 repetitions of 45 seconds with a knee flexion of 60°) immediately reduces pain and cortical motor inhibition, while increasing strength and function.
Eccentric contraction
Eccentric contraction is particularly effective in the treatment of tendinopathies, especially in chronic stages. It helps strengthen the tendon, improve its capacity to bear loads and reduce pain. It stimulates collagen production within the tendon and helps restore muscular and tendinous function.
Manual therapy and osteopathy
Manual therapy and osteopathy play an important role in the management of tendinopathies. In the acute stage, osteopathy may include muscle release techniques and joint mobilisations to improve local blood circulation and movement fluidity. In the chronic stage, manual techniques such as manipulations, muscle stretching and myofascial techniques are commonly used to help restore the function and mobility of the tendon.
Conclusion
Tendinopathies should be addressed in a global manner, with particular attention to associated conditions such as athletic pubalgia or shin splints, taking into account biomechanical or environmental factors (body alignment, stiffness, inadequate sports equipment). Patient involvement is crucial, not only to promote healing but also to ensure treatment adherence. The main objective remains pain reduction and functional recovery. Radiological normalisation is not a priority, as the correlation between imaging and clinical findings is limited.
Frequently Asked Questions
How many osteopathy sessions are needed to treat a tendinopathy?
The number of sessions varies according to the stage of the tendinopathy. In the reactive phase, 2 to 4 sessions may be sufficient. In the chronic or degenerative phase, a protocol of 4 to 8 sessions is generally required, combined with an eccentric strengthening programme.
When should I consult an osteopath for a tendinopathy?
It is recommended to consult as soon as the first symptoms appear: pain on effort, morning stiffness, tenderness on palpation. Early management helps prevent progression to degenerative tendinopathy.
What is the difference between a tendinitis and a tendinopathy?
The term "tendinitis" implies an inflammatory reaction as the main mechanism. Current scientific evidence shows that tendon pain is mainly of degenerative origin, without significant inflammation. The term "tendinopathy" is now preferred in the literature.
Is osteopathy reimbursed for the treatment of tendinopathies?
Osteopathy is not reimbursed by the French national health insurance, but many complementary health insurers cover part of the costs. Check with your health insurance provider.
Can I continue sports during the treatment of a tendinopathy?
A suitable activity is recommended. It is advised to reduce intensity without exceeding the pain threshold. Sustained isometric contraction is particularly beneficial for maintaining activity while controlling pain.
Related articles