Chronic Pain
Myofascial syndrome: chronic muscle pain

Definition and symptoms of myofascial pain syndrome
What is myofascial pain syndrome?
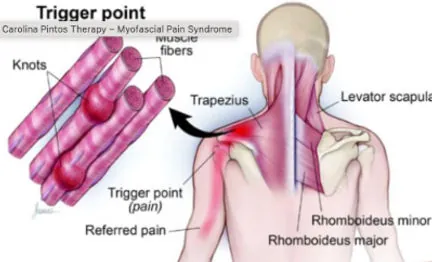
Myofascial pain syndrome is a chronic pain syndrome of the musculoskeletal system characterised by trigger points (TP): small zones of hyperexcitability nestled within a taut muscle band. When stimulated — by pressure, traction or sometimes spontaneously — these points provoke local pain which can radiate to other regions.
Doctors Janet Travell and David Simons, pioneers from the 1950s onwards, formalised the concept of TPs: a hypersensitive zone within an indurated muscle, capable of triggering a specific referred pain for the muscle concerned. They distinguish:
- Active TP: painful at rest or on exertion, it reproduces the typical referred pain of the muscle.
- Latent TP: clinically silent as long as it is not stimulated; pain only appears on provocation.
Although myofascial pain syndrome can be confused with other chronic conditions such as fibromyalgia, it is distinguished from them by the presence of genuine palpable trigger points and pain that is often more localised.
Symptoms of myofascial pain syndrome
The main symptoms include:
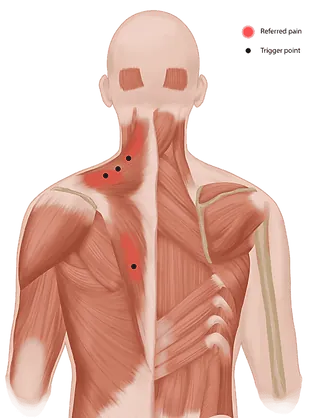
- Localised muscular pain: frequently felt in the neck, shoulders or back
- Active trigger points: sensitive muscular zones that trigger radiating pain when stimulated
- Muscular-origin stiffness
- Fatigue, sleep disturbances
- Headaches
- Postural imbalances
Causes of myofascial syndrome and contributing factors
Myofascial syndrome rarely results from a single cause. The scientific literature identifies a combination of mechanical, neurological and emotional factors that promote the appearance of trigger points and their progression toward chronicity.
Mechanical and postural causes
Repeated strain on muscles is the primary triggering factor. A systematic review with meta-analysis has confirmed the association between sedentary behaviour and cervical and lumbar musculoskeletal pain (Dzakpasu et al., 2021). Prolonged sitting maintains certain muscles in static shortening, creating fertile ground for the local contractures characteristic of myofascial syndrome.
Repetitive movements, sports overuse and unsuitable work postures act through a similar mechanism. When a muscle is worked beyond its recovery capacity, taut bands and painful nodules develop. Biochemical analysis of these zones has shown locally elevated concentrations of inflammatory and algogenic substances, such as substance P, bradykinin and certain cytokines (Shah et al., 2008).
Neurological and emotional factors
Chronic stress and psychological distress are independent risk factors. An umbrella review published in The Clinical Journal of Pain synthesised several systematic reviews showing that depression, anxiety and psychological distress increase the risk of onset and persistence of musculoskeletal pain (Martinez-Calderon et al., 2020).
Sleep deprivation also amplifies the perception of muscle pain, a mechanism now well documented in pain neuroscience (Finan, Goodin, & Smith, 2013). This bidirectional association between sleep and pain explains why patients with chronic muscle pain frequently experience sleep disturbances.
Beyond a certain threshold of chronicity, pain leads to central sensitisation, a phenomenon in which the nervous system amplifies pain perception independently of the initial lesion (Woolf, 2011; Nijs et al., 2021). The muscle no longer carries the condition alone: the spinal cord and brain enter the loop, which changes the therapeutic strategy.
Old injuries and postural compensations
A poorly healed physical trauma (sprain, fall, road traffic accident) can generate lasting postural compensations. The international classification of chronic pain recognises the specific category of chronic post-traumatic pain, which includes musculoskeletal pain persisting beyond the usual healing timeframe (Treede et al., 2019). These compensations load certain muscle groups asymmetrically, favouring the development of trigger points at a distance from the initial injury and fuelling myofascial syndrome.
Diagnosis of myofascial pain syndrome
Clinical diagnosis
The diagnosis is based on a thorough clinical evaluation, as there are no specific imaging tests. The steps include:
- Detailed history: frequency, intensity, triggering and relieving factors of the pain
- Imaging investigations: as needed, to rule out other pathologies
- Observation: detection of postural abnormalities and imbalances
- Physical examination: searching for taut muscle bands and trigger points
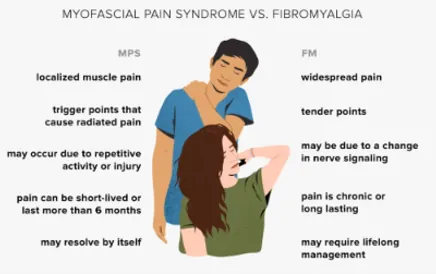
Difference between myofascial pain syndrome and fibromyalgia
- Myofascial pain syndrome: localised and regional pain accompanied by trigger points. Once treated, the pain disappears.
- Fibromyalgia: widespread pain throughout the body, chronic. Fatigue and sleep disturbances are very common.
It is possible for a person to suffer from both conditions simultaneously, making an accurate diagnosis essential.
Treatment of myofascial pain syndrome
Specific injection techniques
The injection of local anaesthetics or corticosteroids into trigger points temporarily numbs the painful zone, reducing local inflammation and thus relieving the immediate pain. These injections are often combined with other techniques to release muscular tension.
Dry Needling
Dry Needling (or "dry acupuncture") consists of inserting fine needles directly into the trigger points of the muscle. This method is effective in relieving muscular pain, reducing tension and improving muscular function.
Osteopathy and manual therapy
Osteopathy plays an essential role in the treatment of myofascial pain syndrome by offering a targeted manual approach. The osteopath uses manual techniques to:
- Inhibit trigger points: relax the muscles affected by trigger points
- Improve blood circulation: promote better oxygenation of muscular tissues
- Restore postural balance: identify and correct the imbalances that contribute to the development of the syndrome
Stretching, mobilisation and self-rehabilitation
Muscular stretches and mobilisations help to release tight muscles and improve flexibility. Patient education and the integration of self-exercises enable better management of pain on a daily basis and prevent recurrence.
Advantages of osteopathy in the treatment of myofascial pain syndrome
- Targeted action on trigger points: ischaemic compression inhibition techniques directly release the trigger points responsible for referred pain. It is the least invasive treatment for myofascial pain syndrome.
- Normalisation of articular mobility: through gentle manipulations (fascial, muscle energy, adapted HVLA techniques), the osteopath restores the mobility of adjacent joints, reducing the tension that maintains the trigger points.
- Comprehensive approach to the patient: myofascial pain syndrome is never isolated. Posture, stress, sleep disturbances or repetitive movements may fuel it. A qualified osteopath explores these factors to provide an adapted response.
- Therapeutic education and ergonomic advice: specific stretching exercises, postural advice at the office, load distribution during sport. This education reinforces the patient's autonomy.

When should you consult an osteopath for chronic muscle pain?
The temporal criterion most commonly accepted is that of the international classification (Treede et al., 2019): pain that persists or recurs beyond three months is considered chronic. Beyond this threshold, the mechanisms involved are no longer purely peripheral. Central sensitisation, the phenomenon by which the nervous system amplifies pain signals, may become established (Woolf, 2011).
Several situations warrant consulting an osteopath specialising in chronic pain:
- chronic muscle pain persisting for more than three months despite rest and conventional treatments
- localised contractures reproducible on palpation, with or without referred pain suggestive of trigger points
- an impact on sleep, concentration or daily activities
- the failure or poor tolerance of a first-line treatment (analgesics, anti-inflammatories, physiotherapy alone)
Certain warning signs should prompt a medical consultation before osteopathic care. Objective loss of strength, persistent tingling, radicular pain following a specific dermatomal path, fever or unexplained weight loss may indicate an underlying cause requiring medical assessment and imaging. Osteopathy then complements the medical care pathway and never replaces it.
At the Victor Hugo Clinic, located at 7 Rue Georges Ville in Paris 16 (Victor Hugo metro station, near Trocadéro), the initial assessment aims to distinguish what falls within osteopathic care from what should be referred elsewhere. When myofascial syndrome is confirmed, manual treatment targets the trigger points and muscle chains involved, with a measurable functional objective.
Appointments are booked via Doctolib.
How many sessions are needed to treat myofascial syndrome?
There is no universal protocol. The number of sessions depends on the duration of the pain, the number of muscles involved and associated factors (sleep, stress, physical activity). The scientific literature nevertheless offers realistic benchmarks.
Acute form (1 to 3 sessions)
When pain is recent (less than six weeks) and linked to an identifiable event (sudden movement, one-off overload), 1 to 3 closely-spaced sessions are often sufficient to restore mobility and deactivate the main trigger points. Clinical trials on manual therapy in musculoskeletal pain report clinically meaningful effects from the very first interventions (Franke, Franke, & Fryer, 2014).
Chronic form (4 to 8 spaced sessions, long-term follow-up)
When chronic muscle pain has been present for more than three months, treatment takes longer. The OSTEOPATHIC randomised controlled trial, conducted in 455 chronic low back pain patients, used a protocol of 6 osteopathic manual treatment sessions over 8 weeks, with effects on pain and function maintained at 12 weeks (Licciardone et al., 2013). Beyond the active phase, follow-up every 4 to 8 weeks may be offered to consolidate gains and prevent recurrence.
Factors influencing prognosis
Several elements modulate the speed of treatment response. The presence of signs of central sensitisation, persistent sleep deprivation, unmanaged chronic stress, as well as psychological factors such as depression and kinesiophobia (fear of movement) lengthen recovery times (Martinez-Calderon et al., 2020; Nijs et al., 2021). Conversely, good sleep hygiene, a gradual return to physical activity and addressing stress factors improve prognosis. No serious osteopath can therefore guarantee a fixed number of sessions without prior assessment.
Prevention and daily habits
Prevention of myofascial syndrome relies on lasting modification of the contributing factors identified in the literature: sedentary behaviour, prolonged static postures, poor stress management and sleep deprivation (Dzakpasu et al., 2021; Finan, Goodin, & Smith, 2013). These levers, modest in isolation, become decisive when combined.
A few simple habits to integrate into daily life to limit the risk of chronic muscle pain recurrence:
- Interrupt static positions every 30 to 45 minutes with a brief mobilisation movement
- Maintain regular sleep of 7 to 9 hours, limiting screens in the evening
- Engage in moderate and regular physical activity, adapted to current capacity
- Identify and address sources of chronic stress (breathing techniques, psychological support if needed)
- Set up your workstation to limit prolonged postural strain
For detailed and tailored exercises, several resources are available: neck stretches, back stretches, back strengthening and office posture. These habits do not replace individualised care by an osteopath in Paris 16, but constitute an essential complement.
Scientific references
- Dzakpasu FQS, Carver A, Brakenridge CJ, Cicuttini F, Urquhart DM, Owen N, Dunstan DW. (2021). Musculoskeletal pain and sedentary behaviour in occupational and non-occupational settings: a systematic review with meta-analysis. International Journal of Behavioral Nutrition and Physical Activity, 18(1), 159.
- Finan PH, Goodin BR, Smith MT. (2013). The association of sleep and pain: an update and a path forward. The Journal of Pain, 14(12), 1539-1552.
- Franke H, Franke JD, Fryer G. (2014). Osteopathic manipulative treatment for nonspecific low back pain: a systematic review and meta-analysis. BMC Musculoskeletal Disorders, 15, 286.
- Licciardone JC, Minotti DE, Gatchel RJ, Kearns CM, Singh KP. (2013). Osteopathic manual treatment and ultrasound therapy for chronic low back pain: a randomized controlled trial. Annals of Family Medicine, 11(2), 122-129.
- Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. (2020). Which Psychological Factors Are Involved in the Onset and/or Persistence of Musculoskeletal Pain? An Umbrella Review of Systematic Reviews and Meta-Analyses of Prospective Cohort Studies. The Clinical Journal of Pain, 36(8), 626-637.
- Nijs J, George SZ, Clauw DJ, Fernández-de-las-Peñas C, Kosek E, Ickmans K, et al. (2021). Central sensitisation in chronic pain conditions: latest discoveries and their potential for precision medicine. The Lancet Rheumatology, 3(5), e383-e392.
- Shah JP, Danoff JV, Desai MJ, Parikh S, Nakamura LY, Phillips TM, Gerber LH. (2008). Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation, 89(1), 16-23.
- Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. (2019). Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain, 160(1), 19-27.
- Woolf CJ. (2011). Central sensitization: implications for the diagnosis and treatment of pain. Pain, 152(3 Suppl), S2-S15.
Frequently Asked Questions
FAQ
What is a trigger point and how does osteopathy treat it?
A trigger point is a hyper-irritated zone within a muscle that causes local and referred pain. The osteopath treats them using ischaemic compression, myofascial stretching and post-isometric relaxation techniques, making it possible to deactivate these painful areas.
What is the difference between fibromyalgia and myofascial pain syndrome?
Fibromyalgia is a generalised condition with widespread pain, chronic fatigue and sleep disturbances. Myofascial pain syndrome is localised to specific muscles with identifiable trigger points. Both conditions can coexist but require different therapeutic approaches.
How many sessions to treat myofascial pain syndrome?
For an acute or recent myofascial pain syndrome, 3 to 5 sessions are generally enough. In chronic forms with numerous active trigger points, 6 to 10 sessions are needed, combined with a daily home stretching programme to maintain the results.
Which muscles are most often affected by myofascial pain syndrome?
The most frequently affected muscles are: the trapezius and the levator scapulae (neck pain and headaches), the quadratus lumborum (low back pain), the piriformis and the gluteal muscles (sciatica), the sternocleidomastoid (dizziness, facial pain) and the masticatory muscles (jaw pain).
Can myofascial syndrome be completely cured?
In most cases, when treatment is initiated before the three-month threshold set by the international classification, complete resolution is possible (Treede et al., 2019). Beyond this point, the outcome depends on the mechanisms involved. If central sensitisation has become established, treatment aims more at lasting symptom reduction than immediate disappearance, through an approach combining manual therapy, gradual return to activity, quality sleep and stress management. The clinical objective is then a return to satisfactory, measurable function, rather than a promise of absolute cure.
Does stress really worsen trigger points?
Yes, and this is not a matter of subjective perception. An umbrella review of systematic reviews has shown that chronic stress, depression and anxiety increase both the risk of onset and the risk of persistence of musculoskeletal pain, independently of mechanical factors (Martinez-Calderon et al., 2020). Stress maintains background muscle tension and impairs sleep quality, two conditions that favour the formation and reactivation of trigger points. The management of chronic muscle pain therefore benefits from addressing these factors.
Why does my myofascial syndrome always come back in the same place?
Recurrences at the same muscle site are explained by the persistence of triggering factors: unchanged work posture, identical repetitive movement, insufficient sleep or chronic stress (Dzakpasu et al., 2021). Locally, biochemical analysis of active trigger points has revealed a persistent inflammatory and acidified environment that maintains muscle sensitivity (Shah et al., 2008). As long as the combination of mechanical and systemic factors is not modified, the vulnerable muscle recovers the conditions that allowed the first flare-up. This is why prevention matters as much as treatment.