Tension headache: mechanisms, diagnosis and treatment
Tension-type headache (TTH) represents the most frequent form of primary headache in the world. TTH is defined by the International Headache Society (IHS) in the 3rd edition of the International Classification of Headache Disorders (ICHD-3) as a bilateral primary headache of mild to moderate intensity, of pressing or constricting quality, non-pulsating, not aggravated by routine physical activity and not associated with nausea or vomiting.
Understanding tension headache
Epidemiology
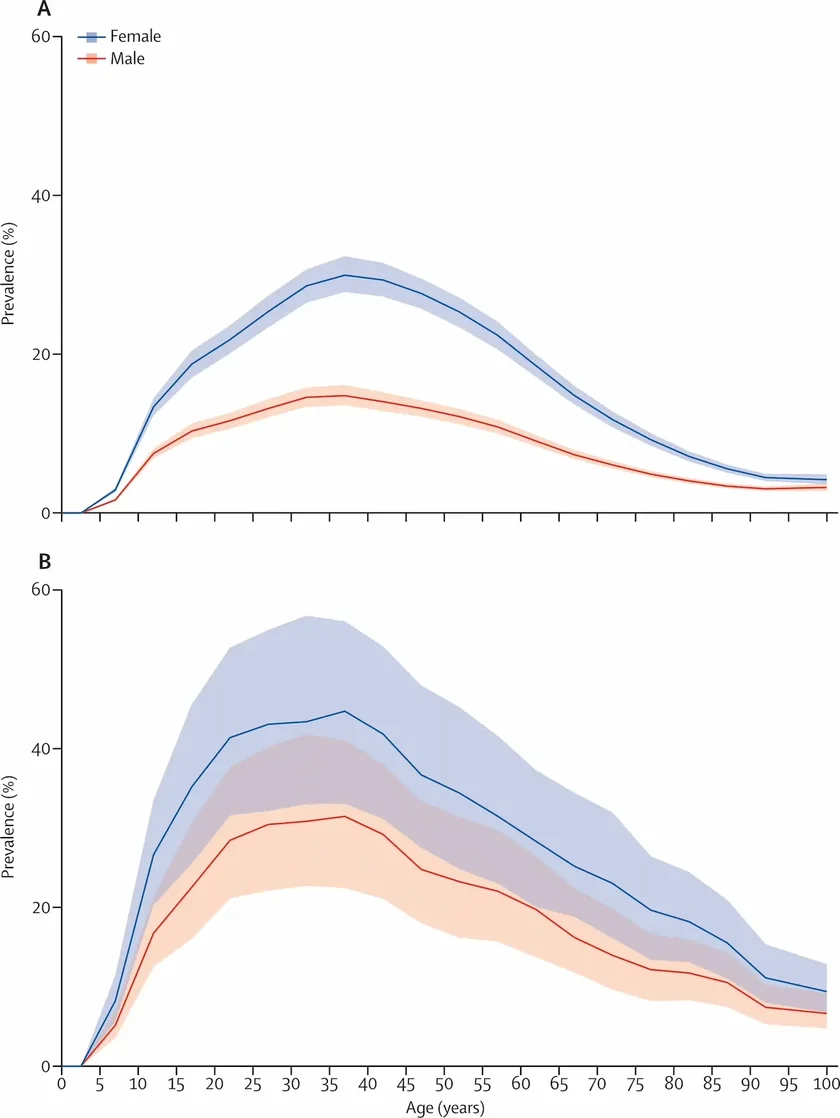
The global prevalence of tension headache is estimated at approximately 26% in adults, with considerable variability depending on the populations studied and study methodologies. It is estimated that 30 to 80% of the adult population will be affected at some point in their lives.
The incidence is higher in women than in men, a difference attributed in part to hormonal factors, stress and psychosocial influences. The burden of TTH, measured in years lived with disability (YLDs), peaks between the ages of 15 and 49.
TTH entails a considerable socio-economic burden. It is associated with more work absences and functional disability than migraine, due to its very high prevalence in the general population.
ICHD-3 classification
The ICHD-3 distinguishes three subtypes of TTH according to the frequency of episodes. This classification directly conditions therapeutic decisions.
| Subtype | Infrequent episodic TTH | Frequent episodic TTH | Chronic TTH |
|---|---|---|---|
| Frequency | < 1 day/month (< 12 days/year) | 1–14 days/month (≥ 3 months) | ≥ 15 days/month (≥ 3 months) |
| Duration | 30 min to 7 days | A few hours to several days | Hours to days, sometimes continuous |
| Functional impact | Low | Moderate to significant | Severe, impairing quality of life |
| Preventive treatment | Not indicated | To be discussed according to impact | Indicated (amitriptyline as first-line) |
Chronic TTH (CTTH) constitutes a distinct entity, characterised by progressive central sensitisation and a more complex therapeutic response.
Clinical picture and diagnostic presentation
Semiological features
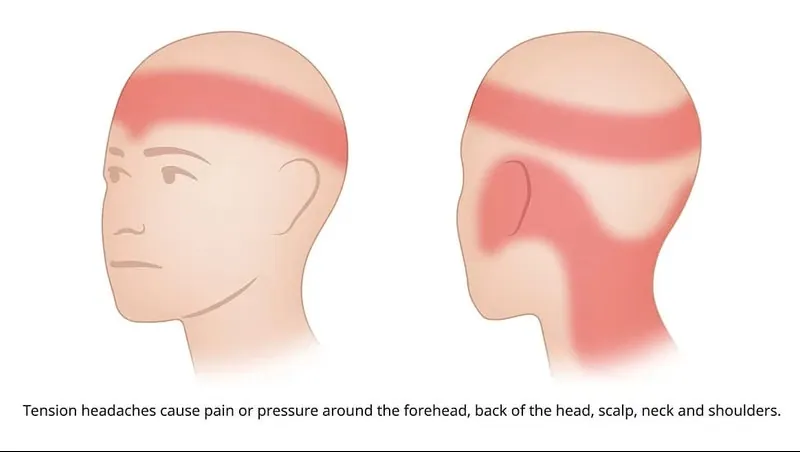
TTH presents as bilateral, diffuse pain of mild to moderate intensity, most often described as a sensation of a helmet, vice or tight band around the head. The pain may radiate to the neck and shoulders. It is non-pulsating and does not worsen with routine physical exertion.
Unlike migraine, TTH is generally not accompanied by nausea or vomiting. Mild photophobia or phonophobia may be present, but never both simultaneously in the episodic form.
ICHD-3 diagnostic criteria
The diagnosis of TTH is clinical, based on history taking and physical examination. Criteria for frequent episodic TTH (2.2):
- At least 10 headache episodes occurring 1 to 14 days/month for more than 3 months
- Duration of 30 minutes to 7 days
- At least 2 of the 4 following features: bilateral location; pressing or tightening (non-pulsating) quality; mild to moderate intensity; no aggravation by routine physical activity
- Absence of nausea and vomiting; no more than one of photophobia and phonophobia
- Not better explained by another ICHD-3 diagnosis
Causes and mechanisms of tension headache
The pathophysiology of TTH is multifactorial and involves an interaction between peripheral and central mechanisms, whose respective weight varies according to the clinical subtype.
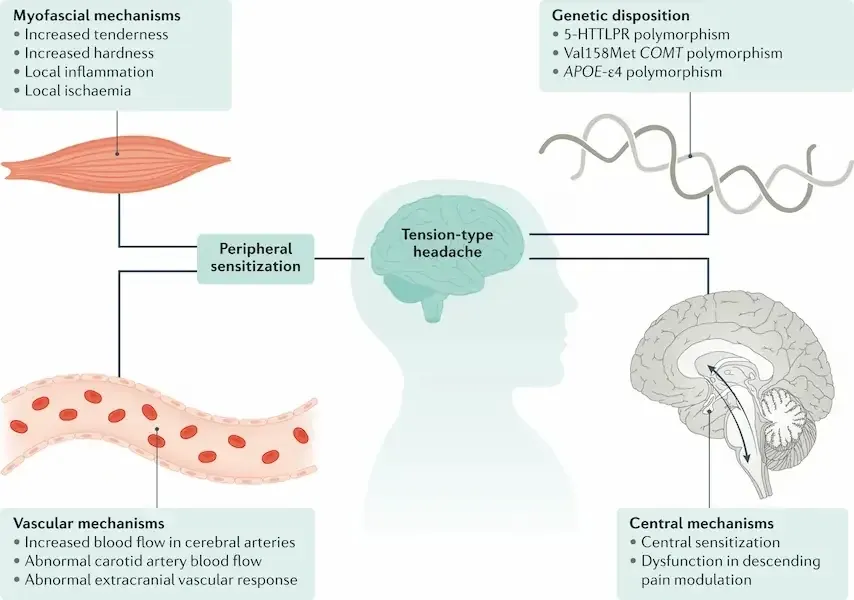
Peripheral mechanisms: myofascial sensitisation
In the episodic forms, pericranial myofascial nociception plays a predominant role. Muscular and connective tissues develop zones of localised sensitivity — myofascial trigger points — which may generate referred pain towards the neck, shoulders and scalp.
Comparative studies have highlighted significantly higher pericranial tenderness in patients suffering from TTH. EMG studies have shown increased muscular activity at rest and reduced recruitment during maximal contractions in patients suffering from CTTH.
Central mechanisms: central sensitisation
The transformation from episodic TTH into CTTH is associated with progressive central sensitisation of second-order neurons. This sensitisation translates into generalised hypersensitivity to pain, both cutaneous and muscular, and an alteration of endogenous pain modulation pathways.
Functional MRI studies have objectively demonstrated modifications of functional cerebral connectivity in patients suffering from TTH. Psychiatric comorbidities — anxiety and depression — are frequently associated with CTTH and contribute to the aggravation of central sensitisation.
Role of stress
Stress constitutes the most frequently reported triggering factor in TTH. The mechanisms involved include activation of neuroendocrine pathways (hypothalamic-pituitary-adrenal axis), chronic muscular tension and alteration of central pain modulation systems.
Risk factors and factors of chronification
- Chronic psychological stress: the leading identified triggering factor
- Sleep disorders: insomnia and obstructive sleep apnoea
- Deficient posture and ergonomics: prolonged work in a static position
- Coexisting migraine: its presence multiplies the risk of chronification
- Psychiatric comorbidities: anxiety, depression
- Overconsumption of analgesics: a major factor maintaining CTTH
Therapeutic management
Treatment of acute attacks
NSAIDs — ibuprofen, ketoprofen, naproxen — and paracetamol constitute first-line treatments. Paracetamol is recommended as a single dose of 500 to 1,000 mg. Triptans, opioids and muscle relaxants are not indicated in the treatment of TTH. Analgesic consumption exceeding 10–15 days per month exposes the patient to the risk of medication-overuse headache (MOH).
Preventive pharmacological treatment
Amitriptyline (a tricyclic antidepressant) represents the reference preventive treatment. Other antidepressants — mirtazapine 30 mg or venlafaxine 150 mg — may be considered as second-line options.
Manual therapies and osteopathy
Manual therapies occupy a validated place in the management of CTTH. A systematic review has shown that manual therapies reduce the frequency of headaches compared with usual care. A meta-analysis published in 2025 in the Journal of Osteopathic Medicine concluded that a combination of osteopathic manipulative treatment techniques effectively reduces the frequency and severity of headaches and improves quality of life.
The documented techniques include work on the trigger points of the pericranial muscles (temporalis, sub-occipital, trapezius, sternocleidomastoid), gentle cervical and thoracic mobilisation and myofascial release techniques.
Complementary non-pharmacological approaches
- Biofeedback: a behavioural technique enabling the patient to modulate their pericranial muscular tension.
- Cognitive behavioural therapy (CBT): indicated in the case of anxiety-depression comorbidities.
- Acupuncture: benefit demonstrated in reducing the frequency of chronic TTH.
- Aerobic physical activity: associated with a reduction in the frequency and intensity of TTH.
- Sleep hygiene and stress management: progressive muscle relaxation, cardiac coherence, mindfulness.
Specific features of managing chronic TTH
CTTH requires a coordinated multidisciplinary approach, combining physician, osteopath or physiotherapist, and if appropriate, a psychologist. The management of an associated MOH requires a progressive withdrawal of analgesics.
Contribution of Charbel Kortbawi DO, MSc.

My specialist osteopathy approach is based on several axes:
- Modulation of central sensitisation mechanisms: through targeted work on cervical, cranial structures and soft tissues.
- Improvement of cervical function and mobility.
- Integrated approach based on the neuroscience of pain: thanks to my MSc in neuroscience, I integrate therapeutic education strategies.
- Personalised self-management strategies: exercises, stress management, ergonomics, physical activity.
Conclusion
Tension headache constitutes the most prevalent primary headache. Its diagnosis relies on precise clinical criteria defined by the ICHD-3 and its treatment draws on a multimodal strategy. The pathophysiology distinguishes peripheral myofascial mechanisms — predominant in the episodic forms — and central sensitisation mechanisms, which are determinant in chronification.
References
- International Headache Society. ICHD-3. Cephalalgia. 2018;38(1):1–211.
- Lee HJ, et al. Update on Tension-type Headache. Headache Pain Res. 2025;26(1):38–47.
- Repiso-Guardeño Á, et al. Does Tension Headache Have a Central or Peripheral Origin? Curr Pain Headache Rep. 2023;27(11):801–810.
- Hager D, et al. Are manual therapies effective at reducing chronic tension headache? J Fam Pract. 2023;72(8):348–355.
- Ashina S, et al. Tension-type headache. Nat Rev Dis Primers. 2021;7(1):24.
- Rehman Y, et al. Osteopathic manipulative treatment in headaches. J Osteopath Med. 2025.
Frequently asked questions (FAQ)
What causes tension headaches?
Tension headaches result from prolonged muscular contractions of the skull, neck and shoulder muscles, often linked to stress, poor posture or visual fatigue. They present as a bilateral sensation of pressure around the head.
Does osteopathy help tension headaches?
Yes, osteopathy reduces the cervical and cranial muscular tensions that underlie tension headaches. Several studies show a decrease in the frequency and intensity of episodes after osteopathic treatment.
How can I quickly relieve a tension headache?
Heat on the back of the neck, a gentle self-massage of the temples and gentle cervical stretches can temporarily relieve the pain. In the long term, osteopathy and stress management are the most effective approaches.
What is the difference between a tension headache and a migraine?
Tension headache is bilateral, of pressing or tightening type, without nausea or sensitivity to light. Migraine is unilateral, pulsating, and often accompanied by nausea, vomiting and photophobia.