Knee pain in athletes: diagnosis and management
Non-traumatic knee pain
Non-traumatic knee pain is common in athletes and represents a major concern for their performance and well-being. Unlike pain of traumatic origin (sprain, fracture, etc.), tendinous and articular knee pain of non-traumatic origin develops progressively and is often due to muscular imbalances, mechanical overload or biomechanical compensations. Rehabilitation, osteopathy and manual therapy play a key role in managing this pain, offering non-invasive treatments based on a holistic approach to the body.

The most frequent knee conditions
- Patellofemoral syndrome (Runner's knee)
Patellofemoral syndrome is one of the most common causes of pain in athletes, particularly those practising running or cycling. It often results from poor load distribution between the patella and the femur, linked to muscular imbalances, poor posture or repeated overload.
Symptoms: Diffuse pain at the front of the knee, aggravated by climbing/descending stairs, running or prolonged sitting.
Treatment: Conservative treatment is favoured, including rest, correction of muscular imbalances (strengthening of the quadriceps, stretching of the hamstrings and the calf), and use of orthopaedic insoles if required.
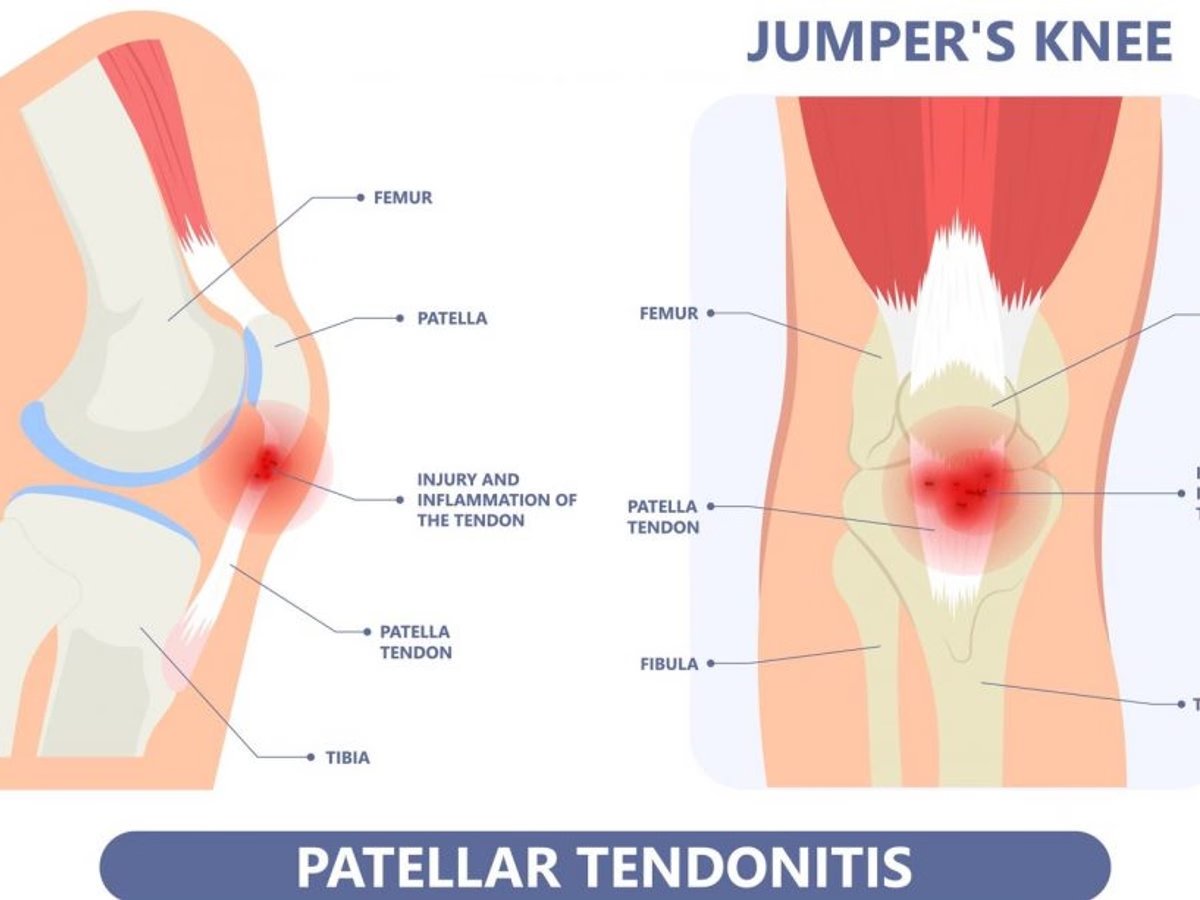
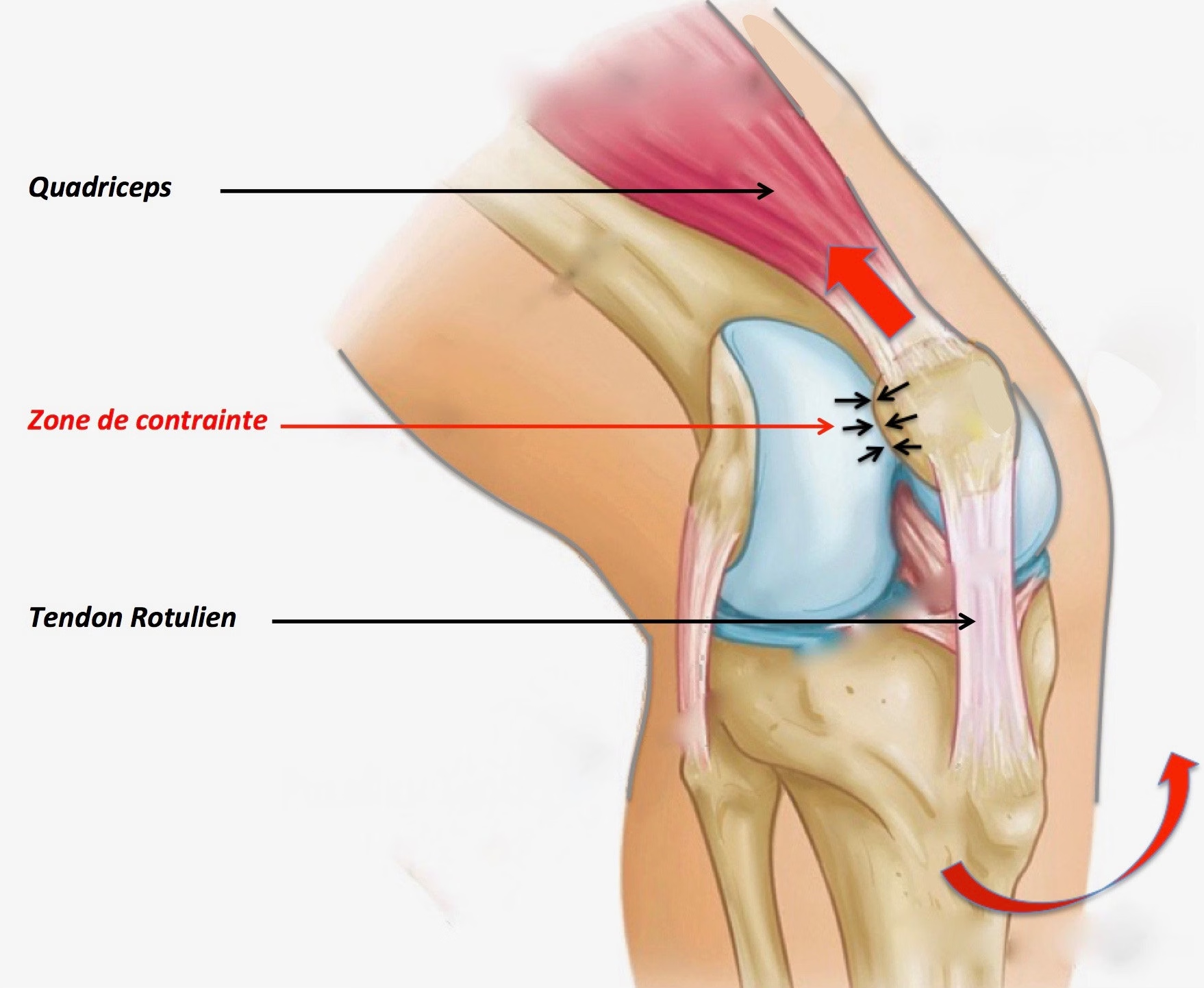
- Patellar tendinopathy (Jumper's knee)
Patellar tendinopathy, nicknamed "jumper's knee", is common in athletes practising sports involving repetitive jumping (basketball, volleyball). It is caused by overuse of the patellar tendon, located just below the patella.
Symptoms: Pain located below the patella, exacerbated by flexion-extension movements of the knee and jumps.
Treatment: Rest and adjustment of sporting activities are essential to reduce overload. Eccentric exercises for the quadriceps are the cornerstone of treatment.
- Iliotibial band syndrome (runner's knee)
This syndrome mainly affects long-distance runners and cyclists. The iliotibial band, a fibrous band running along the outer aspect of the thigh, can rub against the femoral condyle during repetitive flexion-extension movements of the knee, leading to inflammation.
Symptoms: Pain on the outer aspect of the knee, often felt after a few kilometres of running or cycling.
Treatment: Treatment includes specific stretching of the iliotibial band, myofascial massage, and correction of biomechanical factors. Strengthening exercises for the gluteal and core muscles are essential to rebalance the forces applied to the knee.
- Hoffa's syndrome (infrapatellar fat pad impingement)
This syndrome results from inflammation of the adipose tissue located under the patella (Hoffa's fat pad), which may be compressed during knee movements. This syndrome is common in athletes practising sports requiring repetitive deep flexion-extension movements.
Symptoms: Pain located below the patella, often exacerbated by pressure or prolonged flexion movements.
Treatment: Rest, ice and anti-inflammatories are recommended in the acute phase. Rehabilitation aimed at improving mobility and correcting muscular imbalances is paramount.
- Degenerative meniscal lesions
These are lesions that appear progressively over time, rather than being caused by sudden trauma, as is the case for acute meniscal tears. These lesions are often the result of chronic wear of the meniscal tissue and mainly affect older individuals or athletes subjected to repetitive stress on the knees.
Symptoms: Dull pain felt on the inside or outside of the knee, depending on the meniscus affected. Clicking and locking. Moderate swelling. Stiffness and limitation of mobility — patients may experience joint stiffness, with a reduction in range of motion.
Treatment: Non-steroidal anti-inflammatory drugs and corticosteroid injections to relieve inflammation. Muscle strengthening and mobilisations to maintain joint range of motion.
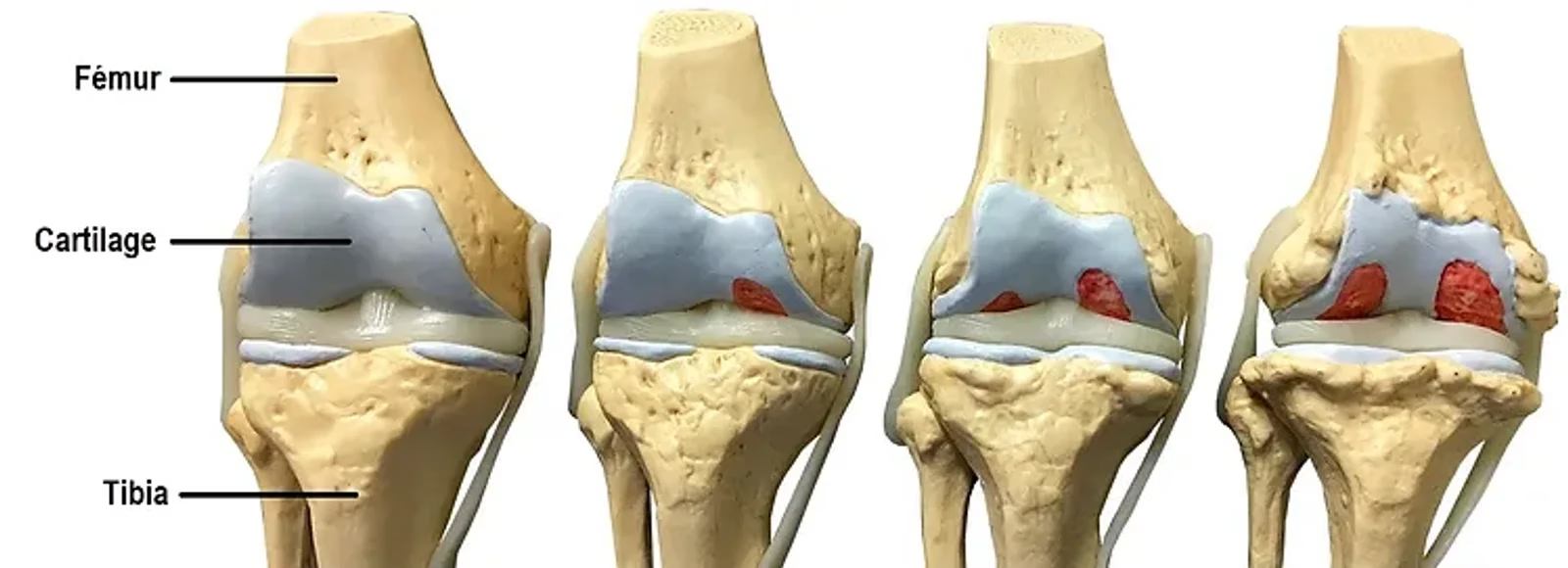
- Knee osteoarthritis (gonarthrosis)
Osteoarthritis is a degeneration of the articular cartilage, which can occur in older athletes or in those with a long history of excessive demand on the knee. Although often linked to ageing, it may appear earlier in athletes due to repeated mechanical overload.
- Symptoms — — Diffuse pain and stiffness at the knee, especially in the morning or after a long period of inactivity. Pain may also occur during or after exercise.
- Treatment — — Management of osteoarthritis includes weight control, moderate exercise, muscle strengthening and maintenance of joint range of motion, as well as the use of orthoses to offload the joint.
Value of osteopathic and manual therapy management
Management through osteopathy and manual therapy relies on a global evaluation of the athlete's body, taking into account postural imbalances, muscular tension and joint dysfunction away from the knee.
Global functional evaluation: The osteopath conducts a comprehensive evaluation to identify restrictions of mobility, postural imbalances or excessive muscular tension that could influence the biomechanics of the knee. Regions such as the spine, pelvis, hips and ankles are systematically examined.
Treatment of mobility restrictions: A restriction of mobility at the pelvis, lumbar vertebrae or ankle can induce compensation at the knee. Gentle mobilisation or manipulation techniques are used to restore normal joint mobility.
Correction of postural imbalances: Postural adjustments can be made to correct imbalances, particularly those affecting the lower limbs. Appropriate postural correction reduces mechanical overload on the knee.
Education and prevention: Patient education is crucial to prevent recurrence. Advice on movement ergonomics, sporting technique, warm-up and stretching, as well as correction of technical gestures (such as running gait), is provided. The osteopath may also offer targeted muscle strengthening exercises for the stabilising muscles of the knee.
Conclusion
Tendinous and articular knee pain in athletes, in the absence of acute trauma, is often due to mechanical overload or muscular and biomechanical imbalances. Treatment relies primarily on functional rehabilitation, relative rest and correction of risk factors. Early and appropriate management helps prevent worsening of symptoms and ensures an optimal return to sport.
Frequently asked questions (FAQ)
Can osteopathy treat knee pain in athletes?
Yes, osteopathy is effective for non-traumatic knee pain (patellofemoral syndrome, iliotibial band syndrome, patellar tendinopathy). It treats the biomechanical imbalances of the hip, knee and ankle that overload the joint.
What are the causes of knee pain in runners?
Frequent causes include: iliotibial band syndrome (runner's knee), patellofemoral syndrome, patellar tendinopathy and bursitis. These conditions often result from progressive overload or muscular imbalance.
Should sport be stopped in the case of knee pain?
Not necessarily. A prompt osteopathic consultation allows the cause to be identified and training to be adapted. Complete rest is often not required; reducing the load and targeted exercises are sufficient in most cases.
How many sessions are needed for sports-related knee pain?
3 to 5 sessions are generally sufficient for non-traumatic knee pain, combined with a muscle strengthening exercise programme. Chronic cases may require longer follow-up.