Tinnitus and osteopathy: what is the link?
Causes, pathophysiology and the contribution of osteopathy and manual therapy in tinnitus. Tinnitus consists of sounds generated spontaneously in the auditory pathway, often subjective, whose origins are varied and sometimes multifactorial. Its pathophysiology is not yet fully elucidated, but significant advances have made it possible to understand some of the mechanisms involved in its appearance. Here is an in-depth look at the origins and pathophysiology of tinnitus as well as the contribution of osteopathy and manual therapy.
1. Origins of tinnitus
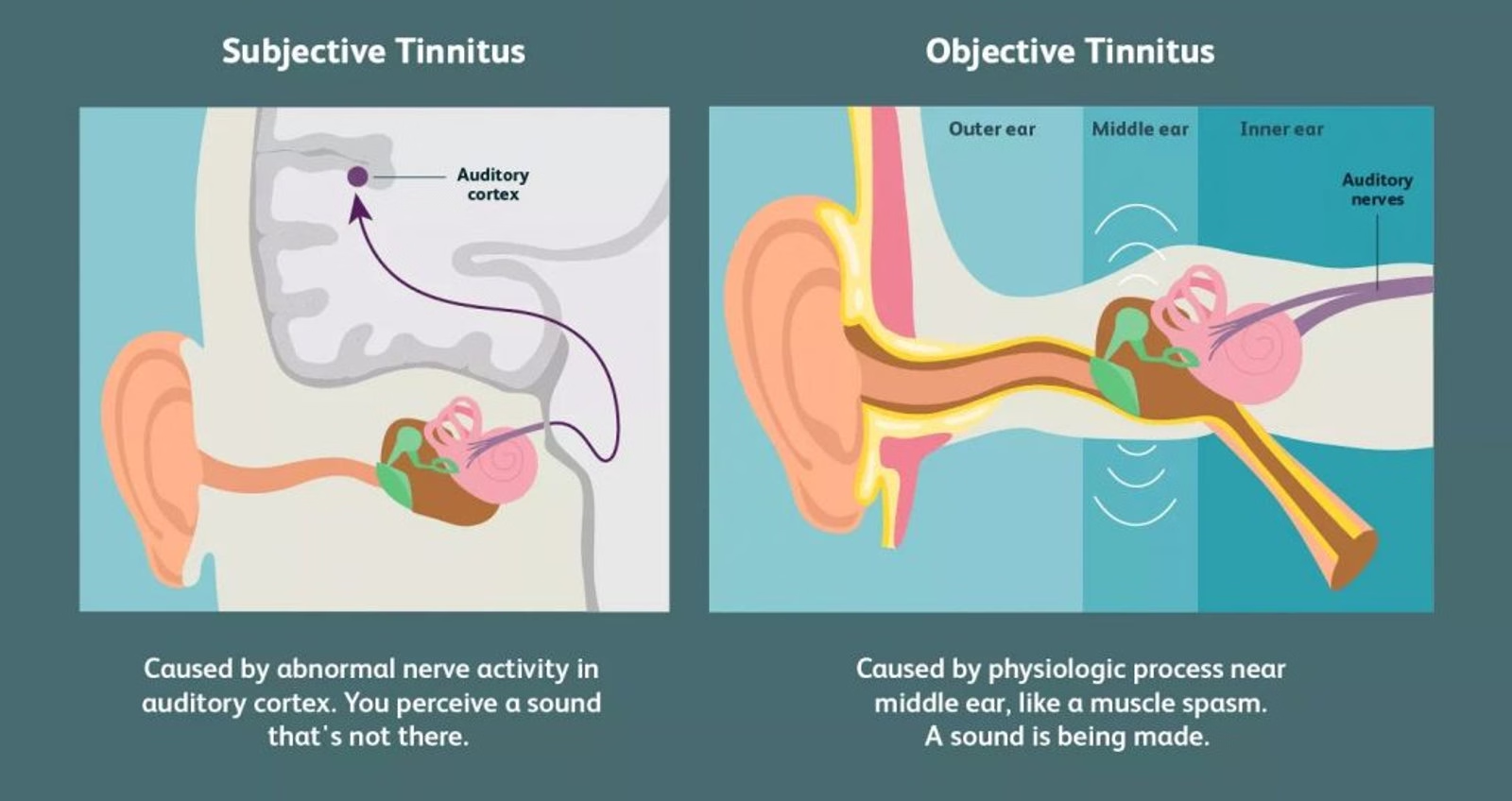
Tinnitus may be classified into two major categories: subjective tinnitus and objective tinnitus. Each of these categories has specific aetiological mechanisms.
Subjective tinnitus is the most common and concerns the majority of patients. It is often associated with pathologies affecting the auditory system, although other factors may also contribute.
- Sound trauma: Prolonged or sudden exposure to high-intensity sounds can damage the hair cells of the cochlea, which are responsible for the transduction of sound vibrations into nerve signals. Once damaged, these cells no longer function correctly, which may lead to hyperactivity of the auditory neurons and the perception of phantom sounds.
- Presbycusis: Age-related hearing loss is another frequent cause of tinnitus. With age, the inner hair cells of the cochlea naturally deteriorate, leading to reduced hearing capacity and, in some cases, the generation of parasitic sounds in the auditory cortex.
- Ototoxicity: Certain medications, such as aminoglycoside antibiotics, loop diuretics or chemotherapy agents (cisplatin), are known to be ototoxic. These substances can cause direct damage to the hair cells of the inner ear, causing tinnitus.
- Temporomandibular joint (TMJ) dysfunctions: A malocclusion or excessive tension of the masticatory muscles can cause tinnitus. The shared innervation between the ear and craniofacial structures via the trigeminal nerve could be a factor explaining the association between these dysfunctions and tinnitus.
Objective tinnitus is rarer and is often caused by real sounds produced by internal body structures, perceptible on clinical examination.
These sounds originate from mechanical, muscular or vascular anomalies that produce real vibrations or sounds captured by the inner ear and sometimes even audible to an outside observer. These sounds may be amplified or modulated by the surrounding anatomy (such as the skull or ear structures).
2. Pathophysiology of tinnitus
The appearance of tinnitus results from an alteration of the auditory system, but also from brain plasticity and neuronal hyperactivity at the level of the auditory cortex and other regions of the brain.
The hair cells of the cochlea, located in the inner ear, play an essential role in the transduction of mechanical signals (sound vibrations) into nerve impulses. When they are damaged (for example following a sound trauma), they lose their ability to correctly filter sounds, which can lead to hearing loss. However, even in the absence of external sound, the auditory neurons continue to generate signals, thus creating aberrant neuronal activity perceived as tinnitus.
Once the hair cells are damaged, cortical reorganisation may occur. The regions of the auditory cortex that normally received sound information from certain frequencies are now under-stimulated. This can lead to hypersensitivity of adjacent neurons and maladaptive reorganisation of the cortical auditory map. This neuronal hyperactivity and excessive synchronisation of neurons in the auditory cortex are considered central mechanisms of tinnitus (Eggermont & Roberts, 2015).
The auditory system includes inhibition mechanisms that filter irrelevant sounds. In tinnitus, it is possible that this inhibition system is altered, leading to an increase in spontaneous activity of the central auditory pathways. This phenomenon of disinhibition could explain why some people perceive tinnitus without any external sound.
Tinnitus is not simply linked to abnormalities of the auditory system, but also involves non-auditory brain circuits, particularly the regions responsible for emotions and attention. The limbic (amygdala, hippocampus) and prefrontal regions are often activated in chronic tinnitus, explaining the link between tinnitus and emotional disorders such as anxiety, depression or insomnia. This model suggests that tinnitus can become a centralised phenomenon, where the brain amplifies perceived sounds through dysfunctional interaction between auditory and non-auditory systems.
Some forms of tinnitus may be influenced by somatosensory inputs from the cervico-facial region. The nerves from the upper cervical ganglia and the craniocervical muscles can modulate the activity of the auditory system. This interaction could explain why certain manoeuvres of the head, neck or jaw exacerbate or relieve tinnitus. This opens up a pathway for management through manual techniques, such as osteopathy.
3. Conventional treatments for tinnitus
There is no single curative treatment for tinnitus, but several approaches aim to relieve symptoms:
- Sound therapy: Exposure to white or natural noises can mask perceived sounds and improve patients' quality of life.
- Medications: Anxiolytics and antidepressants are often prescribed to reduce the anxiety and distress associated with tinnitus.
- Cognitive-behavioural therapy (CBT): These interventions have demonstrated their effectiveness in improving tolerance to tinnitus and reducing psychological impact.
4. Contribution of manual therapy and osteopathy in the management of tinnitus
Osteopathy and manual therapy can offer a complementary approach in the management of tinnitus, particularly when it is associated with somatic and musculoskeletal dysfunctions. Studies have shown that some forms of tinnitus may be linked to muscular tensions or restrictions of mobility at the level of the neck and head as well as at the temporomandibular joint.
Osteopathy can play a role by:
- Managing cervical and muscular dysfunctions: Dysfunctions of the cervical spine, such as stiffness or blockages, can influence tinnitus.
- Managing temporomandibular dysfunctions (TMJ): Temporomandibular joint (TMJ) disorders are frequently associated with tinnitus. Muscular tensions and imbalances of this joint can disturb the cranial and auditory zone.
- Therapeutic patient education.
A systematic review by Sharma et al. (2021) highlighted that manual therapy treatments can help reduce the intensity of tinnitus, particularly in patients presenting associated musculoskeletal tensions.
Conclusion
Tinnitus results from a complex interaction between peripheral factors (auditory trauma, somatosensory dysfunctions, vascular disorders) and central mechanisms involving neuronal plasticity, cortical hyperactivity and the involvement of emotional circuits. The pathophysiology of tinnitus highlights the complexity of the central auditory system and its interaction with other brain regions, which partly explains the difficulty in effectively treating this disorder. The management of tinnitus therefore requires a multimodal approach, integrating medical, behavioural and manual strategies, such as osteopathy, to alleviate the impact of this debilitating symptom.
Frequently asked questions (FAQ)
Can osteopathy help with tinnitus?
Yes, osteopathy can reduce the intensity of tinnitus when it is linked to cervical or jaw musculoskeletal tensions. A systematic review (Sharma et al., 2021) confirms the effectiveness of manual therapies in this context.
How many sessions are needed to treat tinnitus with osteopathy?
On average, 3 to 5 sessions are necessary to evaluate and treat the musculoskeletal components of tinnitus. Results vary according to the origin and duration of symptoms.
What is the difference between subjective and objective tinnitus?
Subjective tinnitus (the most common) is heard only by the patient and often comes from the central auditory system. Objective tinnitus is caused by real sounds produced in the body (vascular or muscular anomalies) and can be heard by an examiner.
Can cervical tensions cause tinnitus?
Yes, cervical muscle tensions and temporomandibular joint (TMJ) dysfunctions are frequently associated with tinnitus. Osteopathy acts directly on these structures to reduce symptoms.