Endometriosis : chronic pain relief
Understanding chronic pain linked to endometriosis
What is endometriosis?
Endometriosis is a chronic gynaecological disease characterised by the presence of endometrial tissue (similar to that which lines the uterus) outside the uterine cavity. The most common locations include the ovaries, the Fallopian tubes, the uterosacral ligaments, the pelvic cavity and sometimes distant organs such as the intestines and lungs. This disease affects approximately 10% of women of reproductive age and is one of the main causes of chronic pelvic pain and infertility.
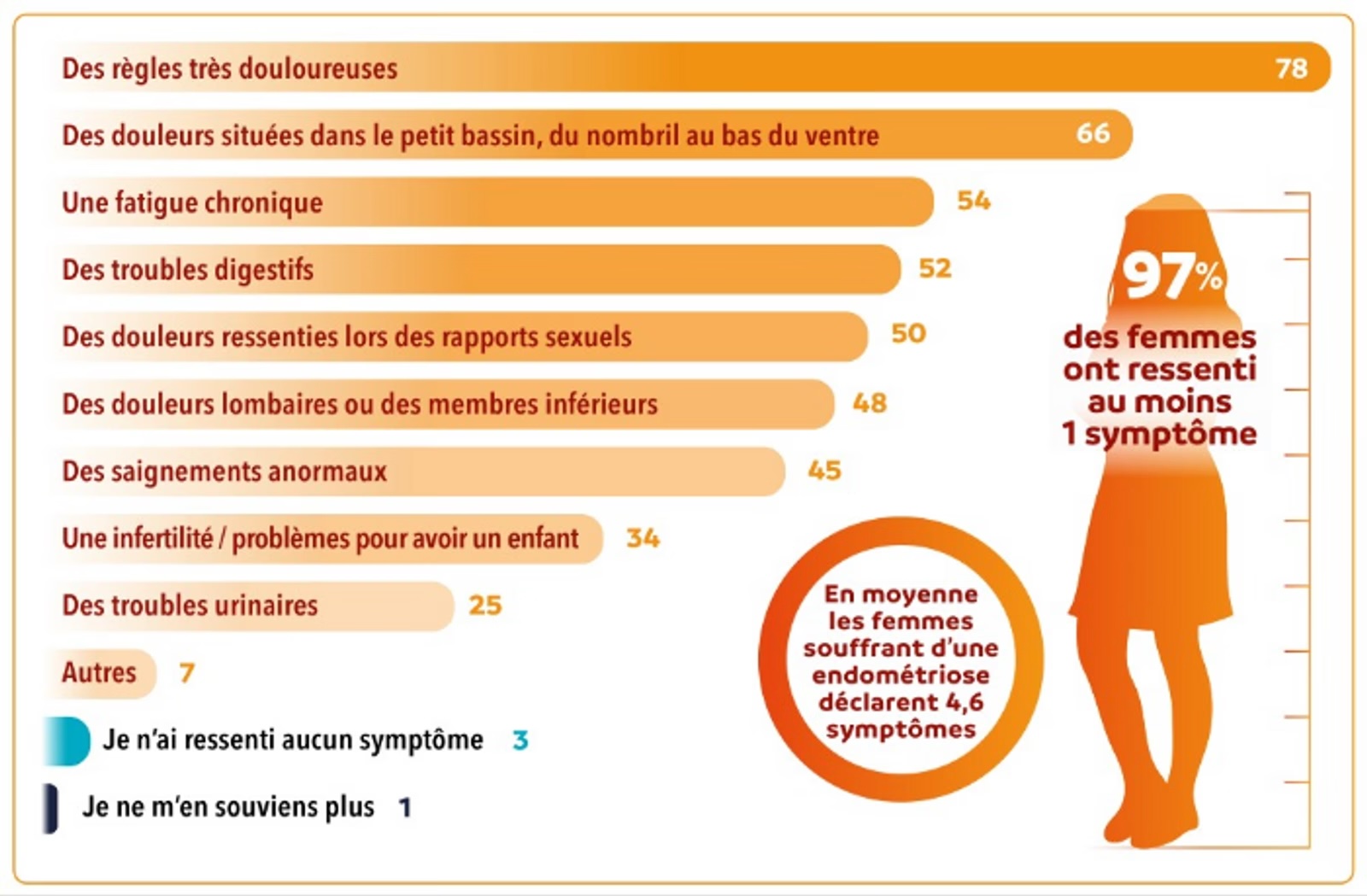
Chronic pain, which can be disabling, is one of the most common symptoms of endometriosis. It affects not only the quality of life of patients, but may also have significant psychological and social repercussions.
Mechanisms of chronic pain in endometriosis
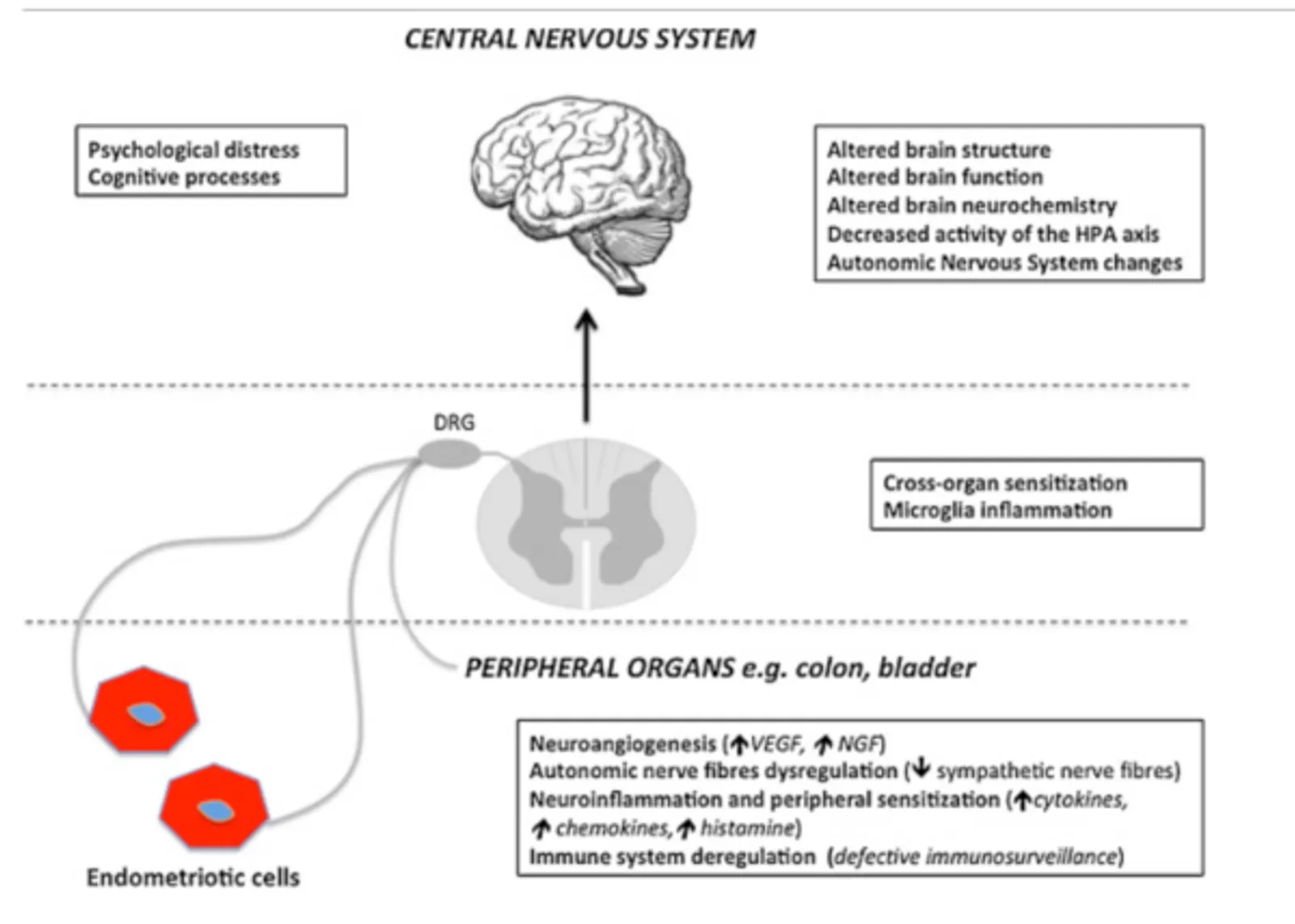
- Lesions and inflammation — Pain linked to endometriosis is multifactorial. One of the first causes is local chronic inflammation. Ectopic endometrial cells respond to the hormonal fluctuations of the menstrual cycle in the same way as the intra-uterine endometrium, that is, by proliferating and then shedding, but with no possibility of evacuation. This leads to microscopic intra-abdominal bleeding, causing peritoneal irritation, an inflammatory reaction and the formation of scar tissue or adhesions. The persistent inflammation is maintained by the release of pro-inflammatory cytokines and growth factors, creating a chronically painful environment.
- Different types of pain — Pain in endometriosis can be classified into several categories:
- Nociceptive pain: caused by the direct stimulation of pain receptors (nociceptors) by inflammation, lesions and adhesions.
- Neuropathic pain: results from nerve injuries induced by endometriotic foci or by repeated surgical procedures. Sensory nerves can become hypersensitive as a consequence of this continued irritation, contributing to chronic pain.
- Central sensitisation: in cases of prolonged endometriosis, a phenomenon of central sensitisation develops. This means that the central nervous system becomes hyperreactive to painful stimuli, amplifying pain sensations, even outside of menstruation periods.
- Psychological and psychosomatic factors
Chronic pain linked to endometriosis can also be exacerbated by psychological factors, notably anxiety, depression and stress. These elements can lower the pain tolerance threshold and contribute to a vicious circle of chronic pain.
Treatment of chronic pain in endometriosis
- Medical and surgical approach
The treatment of endometriosis aims to reduce painful symptoms, control the progression of the disease and improve the quality of life of patients. Here are the most common therapeutic options:
- Hormonal treatments: hormonal treatments aim to stop menstruation and reduce the activity of endometriotic foci. Combined contraceptive pills, progestogens, as well as GnRH (gonadotropin-releasing hormone) analogues are frequently used to induce a temporary menopause.
- Analgesics: non-steroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed to reduce pain. Opioids may be used in severe cases, although their long-term use is limited by the risks of dependence.
- Surgery: in cases where medical treatments are insufficient, laparoscopic surgery can be performed to remove endometriotic lesions and adhesions. Although surgery can offer significant relief, recurrence is frequent.
- Other complementary treatments: nerve injections — nerve blocks or lidocaine injections can be used to relieve neuropathic pain in certain cases.
- Nerve stimulation: techniques such as transcutaneous electrical stimulation (TENS) can help to modulate pain and improve quality of life.
- Osteopathy.
Contribution of manual therapy and osteopathy in the treatment of endometriosis
Manual therapy consists in the use of various techniques for manipulating soft tissues and joints to reduce pain and improve mobility. For endometriosis, these techniques can relieve muscular tensions linked to chronic pain and adhesions, which are often responsible for secondary pain in the pelvic, lumbar and abdominal regions.
- Muscular mobilisations: this type of technique can help to release contracted muscles in the pelvic and lumbar regions, which may reduce pain associated with chronic muscular contractures.
- Releasing trigger points: muscular tensions can lead to the formation of myofascial trigger points (hypersensitive zones within the muscle). Manual techniques aim to reduce these painful points, which can contribute to pelvic pain.
- Visceral manipulations and reduction of fascial tensions: visceral manipulations and myofascial release techniques are techniques used by osteopaths to work directly on the internal organs, notably the uterus, the diaphragm and the intestines. By improving organ mobility, this approach can help to reduce chronic pelvic and abdominal pain linked to endometriosis.
- Whole-body approach: osteopathy also takes an interest in the interactions between the different parts of the body; chronic pain will have repercussions throughout the whole body.
Limits of pain treatments in endometriosis
Endometriosis is often diagnosed late, sometimes after several years of symptoms, which complicates the management of chronic pain. The pain often has time to become established and can be difficult to treat once the disease is advanced.
The pain linked to endometriosis varies from one woman to another, which makes it difficult to propose a standard treatment. Some women respond well to medication or surgical interventions, whereas others continue to experience pain despite treatments. Several studies show that manual therapy and osteopathy can be beneficial for improving the quality of life of patients and relieving the chronic pain associated with endometriosis, especially when integrated into a comprehensive care plan managed by a specialist physician.
Conclusion
Chronic pain linked to endometriosis is the result of complex mechanisms involving inflammation, neuropathy and central sensitisation. There is currently no curative treatment for endometriosis. Treatments aim to control symptoms, but the total elimination of chronic pain remains difficult, particularly due to frequent recurrences.
These limits highlight the need for a multidisciplinary and individualised approach to treat chronic pain linked to endometriosis.
Frequently asked questions (FAQ)
Can osteopathy help with endometriosis?
Osteopathy is a recognised complementary treatment for endometriosis. It acts on pelvic tissue adhesions, tensions of the pelvic floor and postural compensations, thereby reducing associated chronic pain.
Why is the pain chronic in endometriosis?
Endometriosis leads to central sensitisation of pain: the nervous system becomes hypersensitive after months or years of intense pain. This mechanism explains why pain persists even outside of menstruation.
How many osteopathy sessions for endometriosis?
A minimum of 4 to 6 sessions is recommended, ideally outside of menstruation periods. Follow-up is often monthly to accompany hormonal fluctuations and cyclical tissue tensions.
Does osteopathy replace the medical treatment of endometriosis?
No, osteopathy is a complement to gynaecological follow-up, not a substitute. It does not act on endometriotic lesions but significantly improves quality of life by reducing pelvic pain and associated tensions.