Hypermobility and joint pain: when being "flexible" becomes a problem
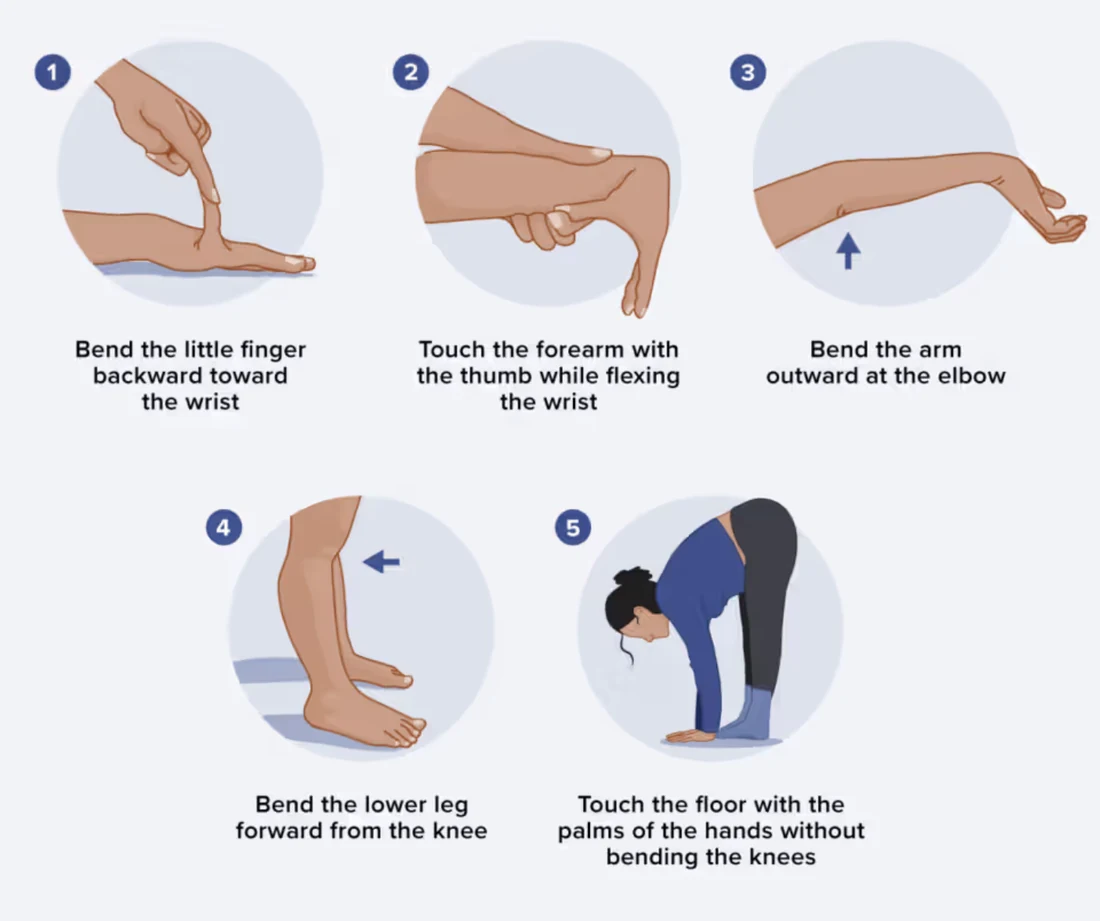
Can you bend your thumb back to touch your forearm? Do your knees or elbows go a little "too far" backwards? For many people this great flexibility is harmless — sometimes even an asset in dance, gymnastics or music. For others, it comes with persistent joint pain, repeated sprains and stubborn fatigue. That is when we talk about symptomatic hypermobility.
Here is what current medical research says about it, without shortcuts or exaggerated promises.
Being hypermobile isn't (necessarily) a disease
Joint hypermobility simply means that some joints move beyond the "normal" range of motion. It is common: studies in students suggest that around 11 to 12.5% of young adults have generalised hypermobility, measured with a standardised test called the Beighton score.
The key distinction is this: as long as it causes no pain, no instability and no other symptom, hypermobility is simply a variation of the human body, not a pathology. The problem begins when it becomes symptomatic — pain, dislocations, frequent injuries, an impact on daily life.
Confusing terminology
If you have looked for information, you have probably come across several names. An international classification published in 2017 brought some order to this vocabulary.
Today, two situations are mainly distinguished in people who are flexible and in pain:
- Hypermobile Ehlers-Danlos syndrome (hEDS), the best-defined form, which meets precise diagnostic criteria.
- Hypermobility spectrum disorders (HSD), a term that covers people with symptomatic hypermobility who do not tick every box for hEDS.
This last term has replaced the older name "joint hypermobility syndrome". Both situations are managed in very similar ways, and researchers still debate whether they are two distinct conditions or a single continuum.
One important point to know: unlike other forms of Ehlers-Danlos, the hypermobile type currently has no identified genetic marker. There is therefore no blood test or DNA test to confirm it — the diagnosis rests entirely on the clinical examination carried out by a doctor.
How is the diagnosis made?
The diagnosis draws on a combination of elements: the Beighton score, which assesses the flexibility of several joints (thumbs, little fingers, elbows, knees and forward bending of the trunk), the history of pain and dislocations, certain skin signs, and above all the exclusion of other connective tissue disorders.
In children and adolescents, the thresholds differ from those in adults, because flexibility is naturally greater at that age. That is why a specifically paediatric diagnostic framework has been proposed: making this diagnosis in a child requires a tailored assessment, not a simple application of the adult criteria.
Why does it hurt?
This is the question most patients ask. Research shows that the pain of hypermobility is multifactorial: several mechanisms combine, and there is no single cause.
Among the documented avenues:
- Direct mechanical pain, linked to excessive loading of overly lax joints, muscles and ligaments.
- A deficit in proprioception (the "position sense" of our joints) and muscle weakness, which leave the joints less well protected.
- A phenomenon called central sensitisation: over time, the nervous system becomes, in a sense, "over-reactive" to pain. A study using fine sensory testing showed that hypermobile patients had lowered pain thresholds and an amplified pain response, with no nerve damage. This pattern is close to what is seen in fibromyalgia.
Understanding this is useful: it explains why the pain can become chronic and diffuse, and why ordinary painkillers are often not enough on their own.
It isn't only about the joints
Hypermobile EDS and HSD are often multisystemic: they can affect far more than the joints. Frequently reported symptoms include fatigue, anxiety, digestive disorders and intolerance of prolonged standing (feelings of faintness, a racing heart).
A few studied examples:
- Digestive disorders: abdominal pain, constipation and bloating are markedly more frequent than in the general population.
- Cardiovascular manifestations: they exist but are most often benign and easy to monitor with cardiac ultrasound.
On the other hand, some associations widely shared online currently rest on weak scientific evidence. This is the case for the "triad" between hypermobility, postural tachycardia (POTS) and mast cell activation (MCAS). It is therefore wise to stay cautious about the categorical claims found online.
What can be done? Movement as the foundation of treatment
There is no curative treatment, but there are real strategies to live better with it. The recognised goals are clear: relieve symptoms, protect the joints and properly understand the condition.
Management rests above all on physiotherapy and tailored physical activity. The available data, even though high-quality trials are still lacking, are encouraging:
- Therapeutic exercise and retraining of muscle function are the approaches with the best evidence of effectiveness. Physiotherapy can improve pain, proprioception and quality of life.
- Muscle strengthening is protective: more toned muscles stabilise overly lax joints.
- Support from a physiotherapist matters a great deal: receiving tailored advice clearly increases the likelihood of taking regular physical activity. Conversely, pain, fatigue and fear of injury are the main barriers to movement — hence the importance of gentle, supervised progression.
Beyond exercise, management is often multidisciplinary: GP, physiotherapist, sometimes occupational therapist, psychological support, and targeted management of digestive symptoms or orthostatic intolerance when present.
Focus: the hypermobile back and back pain
This is a very common scenario in hypermobility spectrum disorders: people who are "flexible in the back", able to place their palms flat on the floor effortlessly, who paradoxically suffer from recurrent low back pain. Many then make an intuitive mistake: thinking that, because they feel stiff or sore at times, they should stretch more or "gain even more flexibility". The data suggest the opposite.

The problem isn't a lack of flexibility — it's too much movement
Hypermobility is associated with an increased risk of back pain. In schoolgirls, the prevalence of hypermobility was significantly higher in those with a history of low back pain.
More importantly, one study measured precisely what happens in a hypermobile lumbar spine: in young hypermobile men (Beighton score ≥ 4), each vertebral level showed an excessive range of motion, and this excess of segmental mobility was associated with more low back pain, more disability and poorer physical function than in controls.
In other words, in a hypermobile back the vertebrae already move "too much" relative to one another. The system is unstable, and it is this instability — not a lack of flexibility — that contributes to the pain.
Why stretching more is rarely the answer
From this observation, the logic becomes clear: gaining still more range on an already over-mobile spine does not correct the underlying problem. What is needed is to restore control and stability to a back that lacks them.
We must be honest about the state of the evidence: to date, no robust study demonstrates that "stretching makes things worse" directly in a hypermobile back. What the data do show is that the proven benefit comes from stabilisation and strengthening, not from increasing mobility. The therapeutic aim is therefore not "more flexibility" but "more control".
What works: stabilise and strengthen
A randomised controlled trial tested exactly this in women with a hypermobility syndrome: an 8-week lumbar stabilisation exercise programme (3 sessions per week) reduced pain intensity, improved trunk muscle endurance and postural stability, while nothing changed in the control group.
More broadly, in instability-related low back pain, patients whose clinical tests reflect segmental instability are precisely those who respond best to a stabilisation exercise programme: the probability of success rose from around 49% to more than 90% in good responders.
In practice, the approach therefore targets:
- core control and the endurance of the deep trunk muscles, to "hold" the spine;
- motor control: learning to move within a controlled range rather than always going to the very end of the joint's range;
- proprioception, that position sense which is often deficient in hypermobile people.
The take-home message for a hypermobile, painful back: the aim is to make it stronger and better controlled, not more flexible. It is counter-intuitive, but it is what the literature points to. Ideally this work is done with a physiotherapist, with gentle progression, all the more so as fear of injury is a real barrier to movement in these patients.
Key points
- Being hypermobile is common and often harmless; it becomes a condition when pain, instability and other symptoms appear.
- The diagnosis of hypermobile EDS is clinical: there is no (genetic) test yet to confirm it.
- The pain has several origins at once, including a possible "hypersensitivity" of the nervous system to pain.
- The condition can affect other systems (digestive, cardiovascular, blood-pressure regulation), but some popular associations lack solid evidence.
- Tailored, progressive movement, supervised by professionals, remains the best long-term ally.
- For a hypermobile, painful back, the aim is stability and control, not more flexibility: the proven benefit comes from stabilisation and strengthening exercises, not from increasing mobility.
If you recognise yourself in this description, the most useful step is to discuss it with a doctor for a structured assessment, rather than self-diagnosing from online information.
Going further
If excessive flexibility comes with back pain that lingers, our page on chronic low back pain sheds complementary light. For the stabilisation work mentioned above, back-strengthening exercises can help, and the role of central sensitisation is detailed on our chronic pain page.
Frequently asked questions (FAQ)
Is hypermobility a disease?
Not in itself. Joint hypermobility is a common variation of the body: around 11 to 12.5% of young adults have a generalised form. As long as it causes no pain, no instability and no other symptom, it is not a pathology. It becomes a condition (symptomatic hypermobility) when pain, dislocations, repeated injuries or an impact on daily life appear.
Is there a genetic test for hypermobile Ehlers-Danlos syndrome?
No. Unlike other forms of Ehlers-Danlos, the hypermobile type currently has no identified genetic marker. There is therefore no blood test or DNA test to confirm it: the diagnosis rests entirely on the clinical examination carried out by a doctor (Beighton score, history of pain and dislocations, and exclusion of other connective tissue disorders).
Why can a very flexible back be painful?
Because the problem is not a lack of flexibility but too much movement. In a hypermobile lumbar spine, each vertebral level shows an excessive range of motion, and this excess of segmental mobility is associated with more pain, more disability and poorer function. It is this instability, not stiffness, that contributes to the pain.
Should you stretch more if you are hypermobile and have back pain?
No, it is often counterproductive. Gaining still more range on an already over-mobile spine does not correct the underlying problem. The proven benefit comes from stabilisation and strengthening (core control, deep trunk muscle endurance, motor control, proprioception), not from increasing mobility. The aim is more control, not more flexibility, ideally with professional support.
A note on the reliability of this article
The content above is based on scientific articles indexed in PubMed (see Sources below). It is intended for general information and does not replace a medical consultation.
Sources (PubMed)
- Malfait F, et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):8-26.
- Castori M, et al. A framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin Med Genet. 2017;175(1):148-157.
- Yew KS, et al. Hypermobile Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorders. Am Fam Physician. 2021;103(8):481-492. PMID 33856167
- Atwell K, et al. Diagnosis and Management of Hypermobility Spectrum Disorders in Primary Care. J Am Board Fam Med. 2021;34(4):838-848.
- Tofts LJ, et al. Pediatric joint hypermobility: a diagnostic framework and narrative review. Orphanet J Rare Dis. 2023;18(1):104.
- Reuter PR, Fichthorn KR. Prevalence of generalized joint hypermobility, musculoskeletal injuries, and chronic musculoskeletal pain among American university students. PeerJ. 2019;7:e7625.
- Zhong G, et al. Prevalence and dynamic characteristics of generalized joint hypermobility in college students. Gait Posture. 2020;82:289-294.
- Syx D, De Wandele I, Rombaut L, Malfait F. Hypermobility, the Ehlers-Danlos syndromes and chronic pain. Clin Exp Rheumatol. 2017;35 Suppl 107(5):116-122. PMID 28967365
- Di Stefano G, et al. Central sensitization as the mechanism underlying pain in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type. Eur J Pain. 2016;20(8):1319-1325.
- Thwaites PA, et al. Hypermobile Ehlers-Danlos syndrome and disorders of the gastrointestinal tract. J Gastroenterol Hepatol. 2022;37(9):1693-1709.
- Rashed ER, et al. Cardiovascular manifestations of hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorders. Vasc Med. 2022;27(3):283-289.
- Kucharik AH, Chang C. The Relationship Between hEDS, POTS, and MCAS. Clin Rev Allergy Immunol. 2020;58(3):273-297.
- Reychler G, et al. Physical therapy treatment of hypermobile Ehlers-Danlos syndrome: A systematic review. Am J Med Genet A. 2021;185(10):2986-2994.
- Brittain MG, et al. Physical therapy interventions in generalized hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome: a scoping review. Disabil Rehabil. 2023.
- Simmonds JV, et al. Exercise beliefs and behaviours of individuals with Joint Hypermobility syndrome/Ehlers-Danlos syndrome - hypermobility type. Disabil Rehabil. 2017;39(14):1432-1440.
- Darakjian AA, et al. Similarities and differences in self-reported symptoms and comorbidities between hEDS and HSD. Rheumatol Adv Pract. 2024.
- Kim HJ, et al. Association of benign joint hypermobility with spinal segmental motion and its clinical implication in active young males. Spine. 2013;38(19):E1013-E1019.
- Noormohammadpour P, et al. The Risk Factors of Low Back Pain in Female High School Students. Spine. 2019;44(6):E357-E365.
- Toprak Celenay S, Ozer Kaya D. Effects of spinal stabilization exercises in women with benign joint hypermobility syndrome: a randomized controlled trial. Rheumatol Int. 2017;37(9):1461-1468.
- Larivière C, et al. Derivation of clinical prediction rules for identifying patients with non-acute low back pain who respond best to a lumbar stabilization exercise program. PLoS One. 2022.
- Larivière C, et al. Disability reduction following a lumbar stabilization exercise program for low back pain. BMC Musculoskelet Disord. 2024.
This article offers general information and does not replace a personalised consultation with a healthcare professional.