Cervicogenic dizziness : relieve vertigo
Definition, causes and management
The entity "cervicogenic vertigo" was first proposed in 1955 by Ryan and Cope to define the causal relationship between cervical involvement and balance disorders. These disorders are rarely of the true vertigo type and the denomination "cervicogenic dizziness" is therefore currently adopted. Cervicogenic dizziness (CD) corresponds to a subjective sensation of imbalance or rotation induced by a dysfunction of the cervical spine.

The main causes of cervicogenic dizziness
- Cervical trauma, notably whiplash-type accidents.
- Chronic poor postures and ergonomic problems.
- Cervical osteoarthritis or degeneration.
- Chronic muscular tensions or spasms of the cervical muscles.
- Cervical disc herniation or dysfunction of the cervical facet joints.
The frequently associated symptoms
- Dizziness triggered or exacerbated by movements of the neck or head.
- Nausea often accompanying the vertiginous episodes.
- Concomitant cervical pain or stiffness.
- Limitation of cervical mobility.
- Headaches of cervical origin, often located at the back of the skull (occipital region).
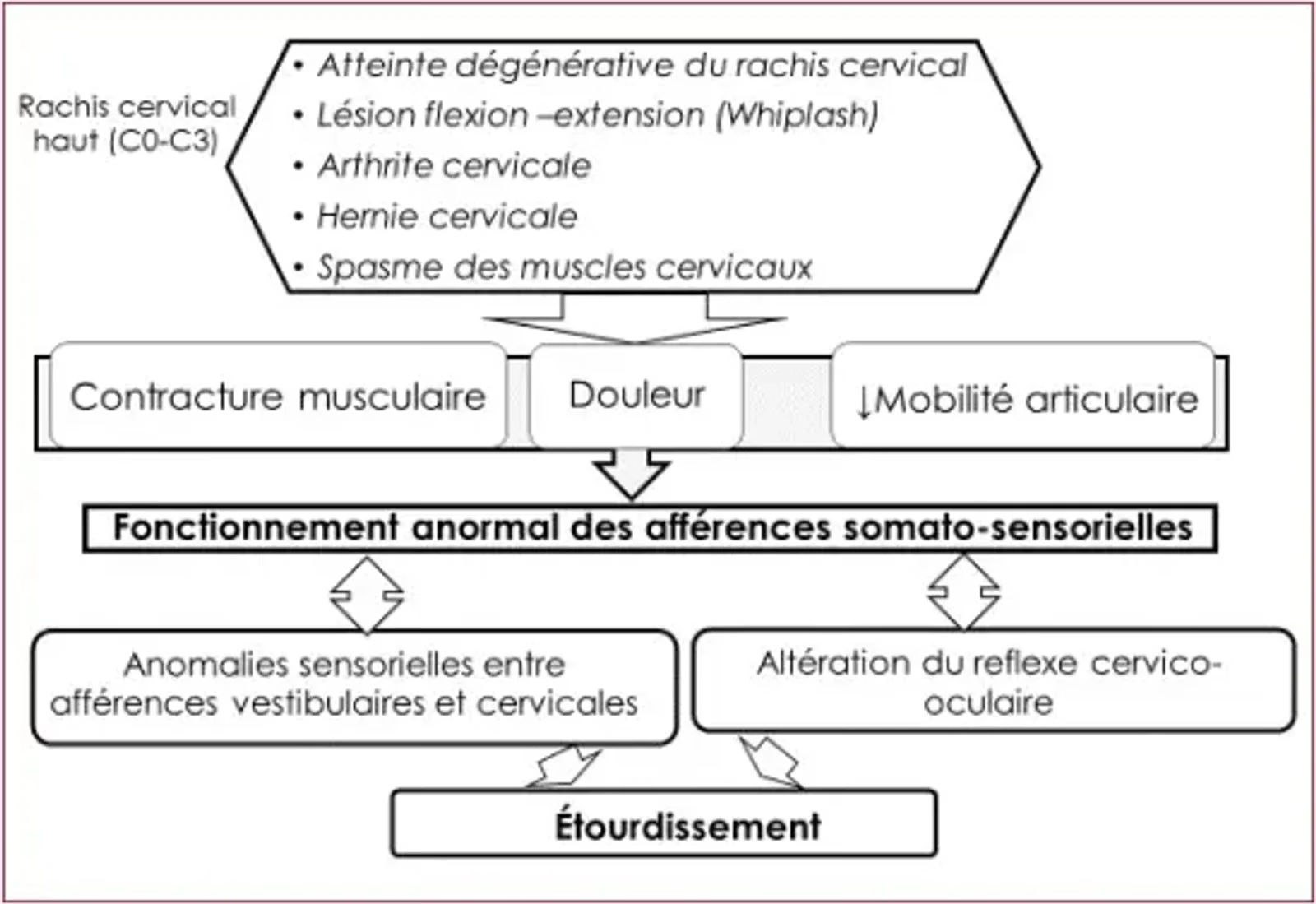
Pathophysiological mechanisms of cervicogenic dizziness
CD is believed to be related to abnormal sensory afferents coming from the damaged proprioceptive receptors of the upper cervical spine (C0–C3). At the current state of knowledge, this theory appears to be supported by solid indirect evidence. It would be at the origin of most CDs. Indeed, it has been demonstrated that the cervical spine and in particular the upper cervical spine C0 and C3 benefits from an exceptional proprioceptive function, being very rich in proprioceptive receptors, both articular and musculotendinous. The somatosensory afferents coming from the affected cervical spine would be asymmetric and discordant compared with the afferents of the other receptor organs, which would be at the origin of the dizziness; the oculo-cervical reflex, indispensable for visual pursuit and recentring of the target on the macula, is altered and therefore the image is no longer stabilised on the retina, which would also be a source of dizziness.
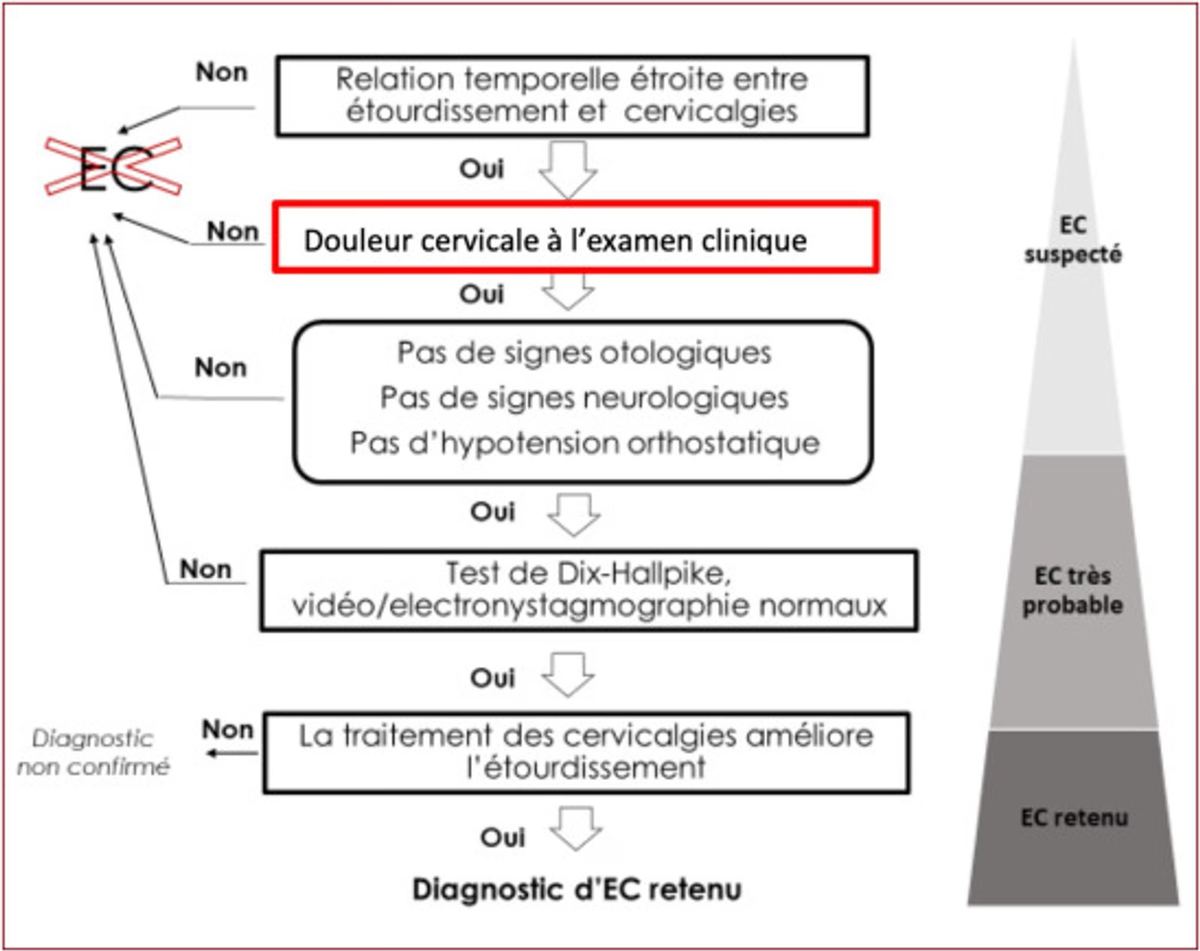
Diagnostic approach
Clinical examination:
- Typically, in the case of CD, the balance disorders are of the dizziness and instability type.
- Precise clinical evaluation including a detailed examination of cervical mobility and of the cervical spine.
- Performance of specific functional tests such as the cervical rotation test or tests assessing the precision of cervical joint repositioning.
Treatment of cervicogenic dizziness
Manual therapy — osteopathy
Manual therapy is the best-studied treatment of cervicogenic dizziness in the literature, with several studies reporting its efficacy.
The aim of the treatment is to restore cervical articular mobility and to rebalance proprioception. The specifically recommended osteopathic techniques include:
- Articular mobilisations
- Myofascial release (MFR)
- Muscle Energy Techniques (MET)
Cervical proprioceptive rehabilitation
Postural control and muscular strengthening exercises are necessary. A strengthening programme for the deep flexor and extensor muscles of the neck would allow better balance of the cervical spine and would increase the proprioception and stability of the head and neck. Oculo-cervical reprogramming should also be offered.
Physiotherapy
Analgesic physiotherapy may be offered (TENS, thermotherapy, muscle-relaxation massage).
Medication
There are no studies having evaluated the efficacy of drug treatment on CD. Data from a retrospective study suggest the efficacy of muscle relaxants, but on the principle that treatments that relieve neck pain also relieve CD, analgesics and non-steroidal anti-inflammatories are also prescribed.
Conclusion
Vertigo of cervical origin is a diagnosis considered in the presence of cervical pain or stiffness associated with sensations of vertigo. It is often linked to a dysregulation of somatosensory afferents through alteration of proprioception receptors at the cervical level. It remains a diagnosis of exclusion in view of the absence of a specific test or imaging examination. Management is multidisciplinary.
- Maatallah K, Cherif I, Ferjani H. Étourdissement cervicogénique : quand cervicalgie et vertige s'intriquent. Douleurs : Évaluation - Diagnostic - Traitement. 2023.
- Guillaume M, Laurin E, Ionescu E. Diagnostiquer le vertige d'origine cervicale. Kinésithérapie, la Revue. 2023.
- Proprioceptive cervicogenic dizziness: a narrative review of pathogenesis, diagnosis, and treatment. J Clin Med. 2022 Oct 26;11(21).
- Cervicogenic dizziness. Oxf Med Case Reports. 2019 Dec 9;2019(11):476-478.
- Proprioceptive cervicogenic dizziness care trajectories in patient subpopulations: a scoping review. J Clin Med. 2023 Feb 27;12(5):1884
Frequently asked questions (FAQ)
Can neck pain cause dizziness?
Yes, cervicogenic dizziness results from tensions and dysfunctions of the neck muscles and joints that disrupt the proprioceptive information sent to the brain. This type of dizziness is often aggravated by head movements.
How does osteopathy treat cervicogenic dizziness?
Osteopathy mobilises the cervical vertebrae, releases sub-occipital muscular tensions and improves cervical proprioception. These techniques reduce dizziness linked to neck dysfunctions in 3 to 5 sessions in the majority of cases.
How can cervicogenic dizziness be distinguished from vertigo?
Cervicogenic dizziness is a sensation of instability or lightheadedness linked to movements of the neck, without rotation of the environment. True vertigo involves a sensation of rotation and is often of vestibular origin (BPPV, Ménière). A medical assessment is essential to differentiate them.
Is cervicogenic dizziness dangerous?
In the vast majority of cases, cervicogenic dizziness is not dangerous. However, any sudden and severe dizziness, associated with visual, auditory or neurological disturbances, requires urgent medical consultation.