Whiplash : treating chronic neck pain
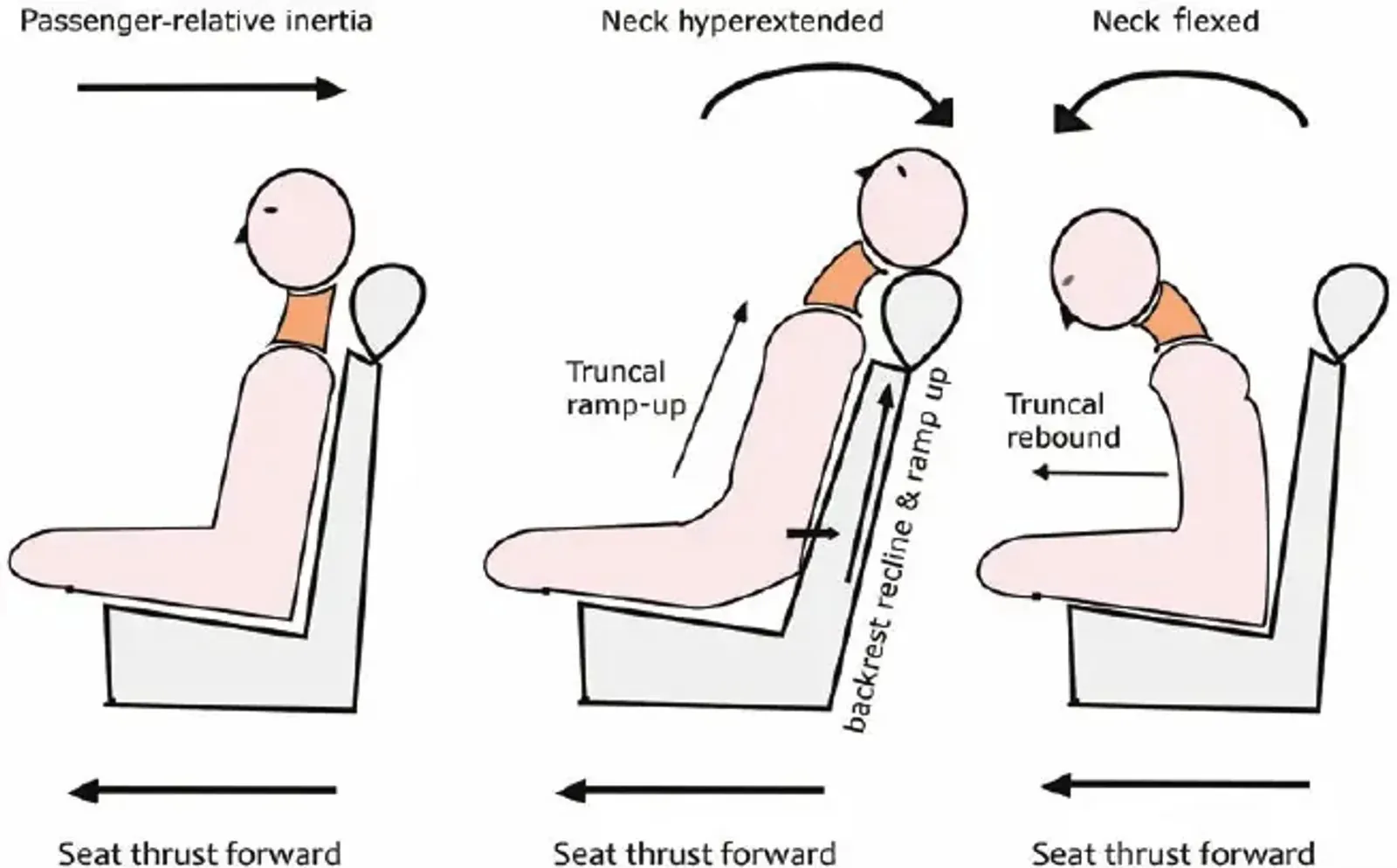
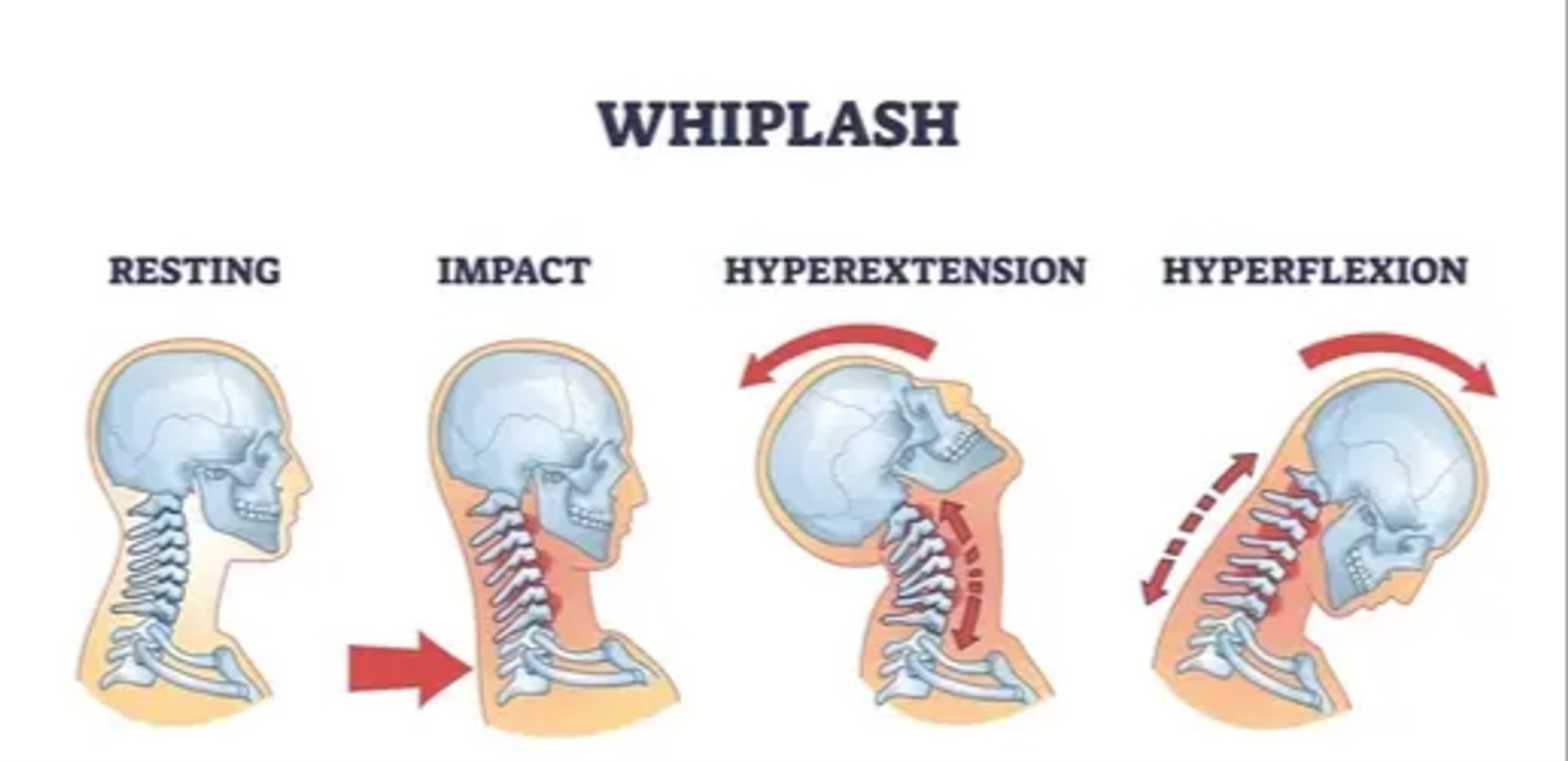
Why does the pain persist and how can it be treated? Introduction Whiplash, medically designated as a cervical acceleration–deceleration injury, occurs most often during motor vehicle accidents, when the neck is subjected to rapid extension–flexion movements. This can lead to lesions of the cervical musculature, ligaments, discs and zygapophyseal joints, sometimes leading to persistent symptoms grouped under the designation of chronic symptoms after whiplash [1].
While many patients recover within a few weeks, a significant proportion — 15 to 50% — develop persistent pain and disability, lasting months or even years [2,3]. Epidemiological studies show that nearly half of the patients suffering from chronic neck pain attribute their symptoms to a previous road traffic accident, underlining the close link between whiplash and chronicity [4].
Underlying mechanisms responsible for the pain
The cervical zygapophyseal joints are well-established contributors to chronic symptoms after whiplash. Studies have shown that facet joint pain is implicated in 74% of patients suffering from chronic symptoms after whiplash. These results were obtained thanks to diagnostic anaesthetic blocks, a technique consisting of injecting a local anaesthetic directly into the cervical joints to identify the exact source of the pain, and done in a placebo-controlled manner to confirm that the pain does indeed come from the targeted joints [5].
However, the cervical muscular structures also play an essential role in the persistence of post-traumatic pain. Direct muscular lesions, microtears and secondary fibrosis can lead to local sensitisation and chronic pain. Furthermore, numerous works have shown the presence of myofascial trigger points in the cervical muscles (notably the upper trapezius, the sternocleidomastoid and the deep flexor muscles of the neck) in patients suffering from chronic symptoms after whiplash [6]. These painful points contribute not only to local pain, but also to referred pain phenomena and to the restriction of cervical mobility.
Imaging studies, notably by MRI and ultrasound, have also revealed structural and functional modifications of the cervical muscles after an acceleration–deceleration trauma: fatty infiltration, alteration of neuromuscular control and decrease in muscular endurance and strength [7]. These alterations may explain the tendency towards chronification and the difficulties of complete recovery in some patients.
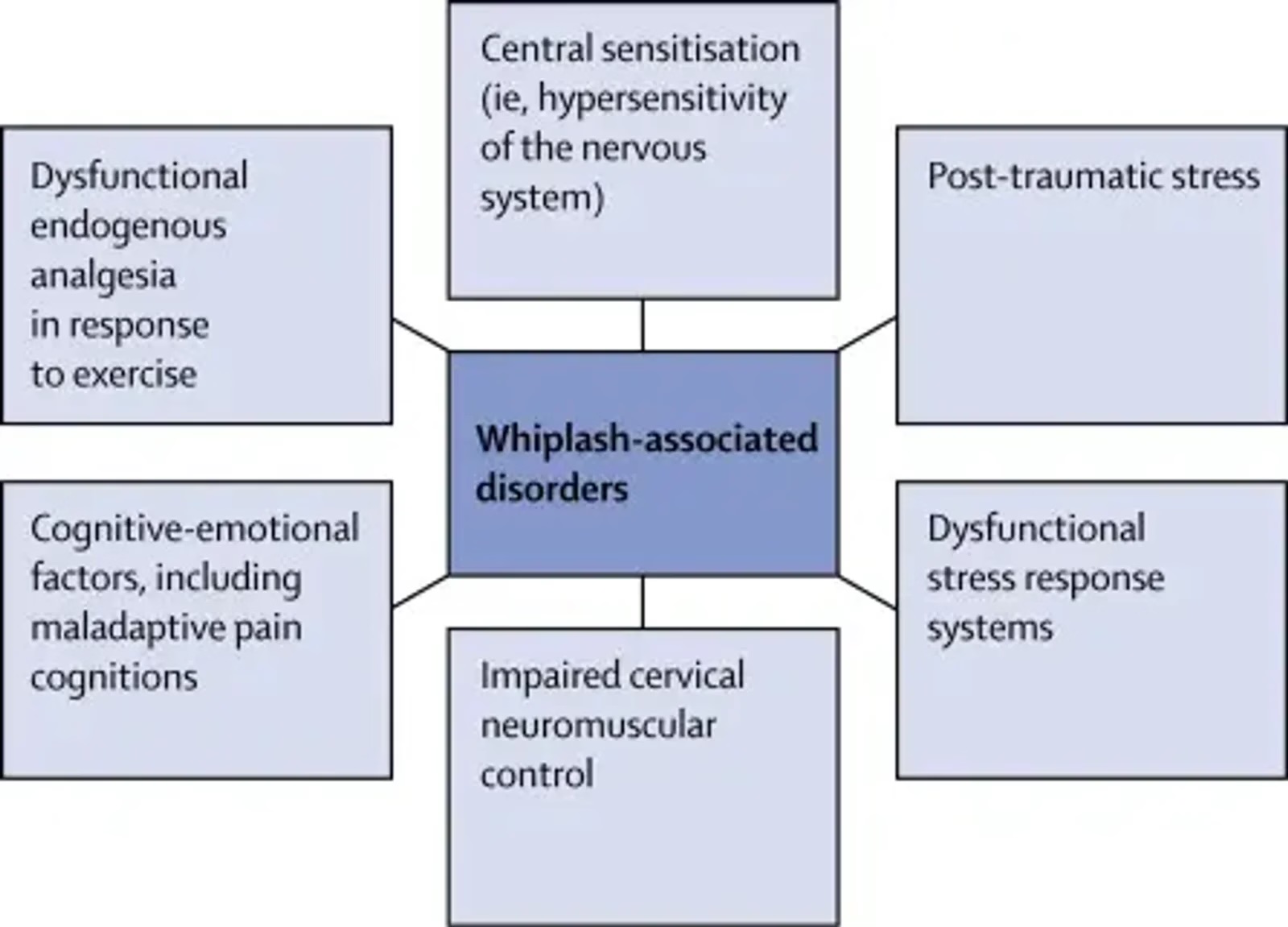
Chronic symptoms after whiplash are not explained solely by peripheral lesions. Research has shown that sensory hypersensitivity appears very early after the injury and is associated with an unfavourable recovery [6]. This phenomenon, called central sensitisation, corresponds to an amplification of pain signals by the central nervous system, even in the absence of detectable tissue lesions. It may provoke persistent pain, exaggerated or triggered by normally painless stimuli [6].
Psychological and cognitive factors also play a major role in the evolution of symptoms. A prospective study has shown that an intense initial pain and a high level of catastrophising (the tendency to anticipate the worst and to amplify the negative consequences of pain) are strongly associated with the development of post-traumatic headaches after whiplash, with catastrophising increasing the risk significantly (x15) [7]. These data underline the importance of early evaluation of pain-related beliefs and coping strategies from the acute phase.
Finally, the impact of whiplash on patients' daily life is considerable. A qualitative study of 349 patients showed that this condition modifies body perception, disrupts daily life and influences the recovery trajectory of chronic patients
[8]. This illustrates the profound biopsychosocial impact of whiplash and underlines the need for appropriate therapeutic approaches.
Treatment and management of chronic neck pain: evidence and recommendations
Manual therapies (osteopathy) and physical rehabilitation
Data from the OPTIMa protocol (Ontario Protocol for Traffic Injury Management) and other recommendations indicate that manual therapy (mobilisation/manipulation) is beneficial in acute and chronic post-whiplash neck pain of grades I–II [9].
Supervised muscular strengthening exercise programmes are also beneficial and recommended for patients.
On the other hand, passive modalities such as ultrasound, diathermy, hydrotherapy and certain acupuncture approaches show limited or no benefit and are not recommended as isolated interventions [9].
Rehabilitation based on pain neuroscience
Modern rehabilitation approaches focus on the central mechanisms of pain. A major randomised clinical trial in 2025 showed that an approach combining pain education, stress management and cognitive exercises, carried out contingently, led to superior improvements in terms of disability, central sensitisation and kinesiophobia, compared with usual care. The MPNA group also presented better cost-effectiveness and a higher probability of improvement after treatment [11].
Complementary data concerning chronic non-specific neck pain confirm that the combination of pain education + exercise more effectively reduces disability, catastrophising and fear of movement than exercise alone [12].
Interventional approaches
In patients suffering from pain of facet origin, medial branch blocks and radiofrequency neurotomy remain validated interventional strategies, often allowing significant pain relief and functional improvement [5].
Clinical implications
- Early identification of risks: intense initial pain and catastrophising are powerful predictors of poor prognosis; their early screening allows targeted intervention [7].
- Multimodal management: the optimal approach combines education, active rehabilitation, manual therapy and, if indicated, targeted interventions.
- Avoiding low-value care: passive modalities without solid evidence should be limited in favour of active and patient-centred approaches [9].
- Taking central mechanisms into account: the integration of pain education, stress management and cognitive-behavioural principles helps target central sensitisation and maladaptive beliefs [11,12].
- Patient-centred biopsychosocial approach: recognising and treating the patients' lived experience is essential for overall recovery [8].
Conclusion
Chronic post-whiplash neck pain is multifactorial, resulting from both peripheral mechanisms (e.g. facet joint pain) and central processes (e.g. sensitisation, psychological distress). Current evidence clearly favours active and individualised management. Early identification of at-risk patients and the setting up of multimodal management are essential.
Personally, I combine in my treatment:
- Manual therapy and osteopathy
- Thanks to my diplomas and training in neuroscience and pain management, therapeutic education, pain management strategies and rehabilitation centred on neurophysiological mechanisms, in order to offer comprehensive and personalised treatment to each patient.
References
- Sterling M. Physiotherapy management of whiplash-associated disorders (WAD). J Physiother. 2014;60(1):5–12. PMID: 24503214.
- Carroll LJ, — Holm LW, Hogg — Johnson S, et al. Course and prognostic factors for neck pain in whiplash-associated disorders (WAD). Spine (Phila Pa 1976). 2008;33(4 Suppl):S83–92. PMID: 18204389.
- Walton DM, — MacDermid JC, Giorgianni AA, et al. Risk factors for persistent problems following acute whiplash injury: update of a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2013;43(2):31–43. PMID: 23322093.
- Freeman MD, — Croft AC, Rossignol AM. Whiplash associated disorders: redefining whiplash and its management. Spine (Phila Pa 1976). 1998;23(9):1043–9. PMID: 9580931.
- Lord SM, — Barnsley L, Wallis BJ, Bogduk N. Chronic cervical zygapophysial joint pain after whiplash. A placebo-controlled prevalence study. Spine (Phila Pa 1976). 1996;21(15):1737–45. PMID: 8855458.
- Sterling M, — Jull G, Vicenzino B, Kenardy J. Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery. Pain. 2003;104(3):509–17. PMID: 12927623.
- Thorn P, — Nicholson B, MacDonald L, et al. Higher Neck Pain Intensity and Pain Catastrophizing Partially Explain Persistent Posttraumatic Headache with Whiplash. Clin J Pain. 2024;40(6):349–55. PMID: 38465710.
- Crestani M, — Cook C, Ceccarelli E, et al. “I’m Not the Same as I Was Before”: A Qualitative Evidence Synthesis Exploring the Experiences and Perceptions of Patients Living With Whiplash-Associated Disorders. J Orthop Sports Phys Ther. 2025;55(9):1–19. PMID: 40879621.
- Wong JJ, — Shearer HM, Mior S, et al. Are manual therapies, passive physical modalities, or acupuncture effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? Spine J. 2016;16(12):1598–1630. PMID: 26707074.
- Peters R, — Hallegraeff J, Koes B, van Trijffel E. Recommendations for Mobilization and Manipulation Treatment and Screening for Vascular Complications in Clinical Practice Guidelines for Neck Pain: A Systematic Review. Phys Ther. 2025;105(2):pzae179. PMID: 39791243.
- Malfliet A, — Lenoir D, Murillo C, et al. Pain Science Education, Stress Management, and Cognition-Targeted Exercise Therapy in Chronic Whiplash Disorders: A Randomized Clinical Trial. JAMA Netw Open.2025;8(8):e2526674. PMID: 40794407.
- Lluch — Girbés E, et al. Pain neuroscience education and exercise for chronic neck pain: a randomized controlled trial. Int J Environ Res Public Health. 2021;18(16):8848. PMID: 34444734.
Osteopath — Chronic Pain Management — Sport
French Diploma of Osteopathy
Further reading : cervicogenic dizziness.
Frequently asked questions (FAQ)
Does osteopathy help after a whiplash?
Yes, osteopathy is one of the best-documented treatments for whiplash. It reduces cervical muscular tensions, restores the mobility of the vertebrae and treats the postural compensations resulting from the trauma. Early management improves the prognosis.
Why does pain persist after a whiplash?
The persistence of post-whiplash pain is explained by central sensitisation of the nervous system: after the trauma, the pain circuits remain activated even after tissue healing. Therapeutic education and osteopathy are essential to break this cycle.
How soon after an accident can you see an osteopath?
It is recommended to consult within 48 to 72 hours following the accident (after medical and radiological assessment). Early management reduces the risk of chronification of post-traumatic cervical pain.
What are the symptoms of an untreated whiplash?
An untreated whiplash can evolve into chronic neck pain, headaches, dizziness, concentration and memory disturbances. In 10 to 15% of cases, the symptoms persist for more than a year in the absence of appropriate management.