Sciatica: differential diagnoses and common causes of leg pain
Sciatica is not a disease, but a symptom
"I've got sciatica." The phrase is used all the time when pain begins in the buttock and travels down toward the thigh, calf or foot. Yet the term "sciatica" does not name a disease as such. It describes a symptom: pain radiating into the lower limb along the path of the sciatic nerve or its nerve roots.
This distinction is essential. Behind pain that runs down the leg may lie very different mechanisms: irritation of a lumbar nerve root, involvement of the deep structures of the gluteal region, referred pain arising from the lumbar spine, or narrowing of the lumbar canal.
The aim of the differential diagnosis is precisely to identify the true origin of the symptoms, so that management can be directed appropriately. When pain radiates into the leg, the point is therefore not simply to label it "sciatica," but to understand what is actually causing it.
True sciatica: when the nerve is genuinely involved
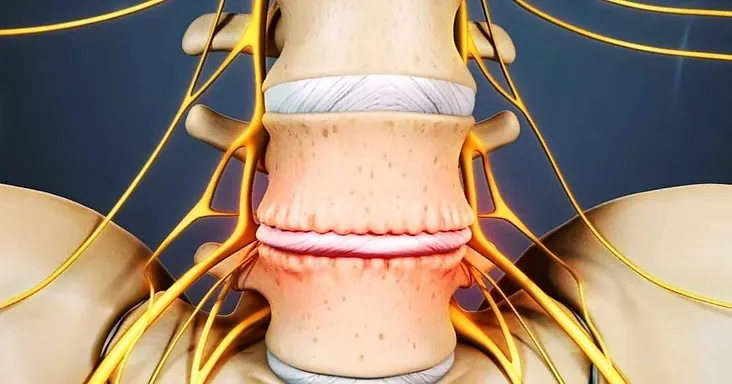
In the medical sense of the term, sciatica corresponds to radicular pain related to involvement of a lumbar or sacral nerve root, most often L5 or S1. The most common cause is a lumbar disc herniation, which can irritate or compress a nerve root as it leaves the spinal column.
The pain usually begins in the lower back or gluteal region before extending into the lower limb. It may be accompanied by suggestive neurological manifestations:
- tingling;
- numbness;
- electric-shock sensations;
- reduced sensation;
- muscular weakness affecting certain movements of the foot or leg.
The pain generally follows a territory consistent with the nerve root involved, even if some presentations may be atypical.
In most cases, the course is favourable over time with appropriate care. The clinical examination makes it possible to confirm the nerve origin of the symptoms, assess their functional impact, and rule out other causes of pain radiating into the lower limb.
"False sciatica": when pain mimics nerve involvement
Not all pain that runs down the leg is related to nerve compression. Several conditions can reproduce symptoms very close to those of sciatica.
Deep gluteal syndrome
The sciatic nerve crosses the deep region of the buttock before reaching the back of the thigh. Irritation or compression of the nerve by the structures located in this anatomical space can cause pain resembling sciatica.
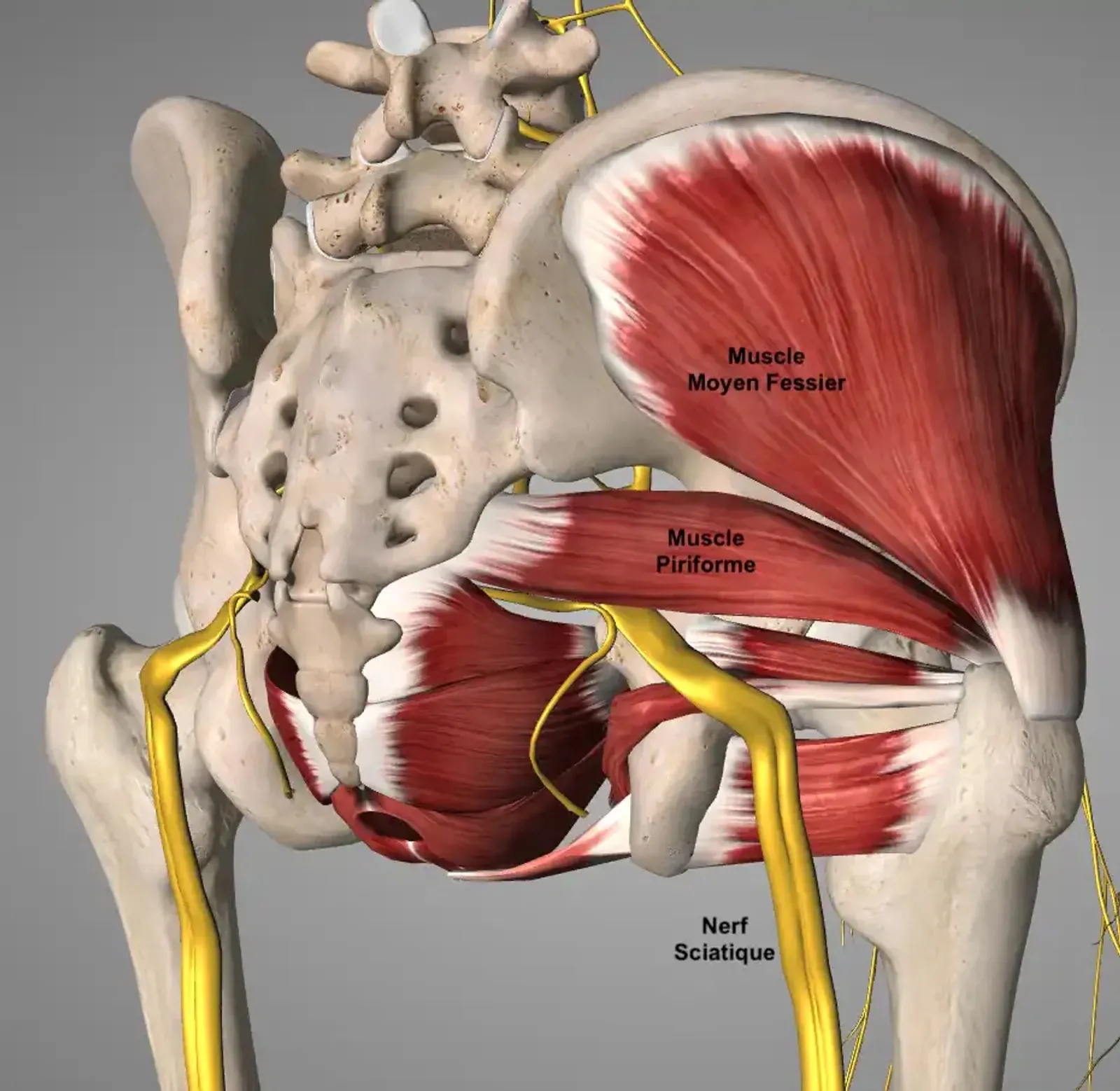
This situation is now grouped under the term deep gluteal syndrome, which encompasses what was formerly called piriformis syndrome. Indeed, several structures may be involved, not only the piriformis muscle.
The symptoms are often characterised by:
- deep pain in the buttock;
- worsening with prolonged sitting;
- radiation toward the back of the thigh;
- discomfort during certain sporting activities or while walking;
- the frequent absence of objective neurological signs.
In our osteopathic practice at the Cabinet Victor Hugo in Paris 16, it is not uncommon to see patients convinced they have sciatica when the origin of their symptoms lies in the deep structures of the gluteal region.
Referred pain from the lumbar spine or pelvis
Certain anatomical structures are able to project pain at a distance without any true nerve involvement.
This is notably the case for:
- the lumbar facet (zygapophyseal) joints;
- the intervertebral discs;
- the sacroiliac joint;
- certain muscular structures of the lumbopelvic region.

The pain may be felt in the buttock or thigh, sometimes as far as the knee. Unlike radicular pain, it is generally less well systematised and does not correspond to a precise neurological territory.
Lumbar canal stenosis
In older people, progressive narrowing of the lumbar canal can lead to compression of the nerve structures.
The clinical picture is often characteristic:
- pain or a sensation of heaviness in the legs when walking;
- a progressive reduction in walking distance;
- worsening with prolonged standing;
- improvement of symptoms when sitting or when the trunk is bent forward.
This situation is called neurogenic claudication. It differs from sciatica related to a disc herniation and requires specific management.
Warning signs: when to seek care quickly
Most pain radiating into the leg is benign and follows a favourable course. Some signs should nonetheless prompt a rapid consultation:
- difficulty passing urine or controlling the bowels;
- loss of sensation in the genital or perineal region;
- significant or rapidly worsening muscular weakness;
- pain associated with fever or a deterioration in general condition;
- pain appearing after a major injury;
- severe, persistent pain, particularly at night.
These situations may suggest a condition requiring urgent care, in particular cauda equina syndrome.
How is the diagnosis made?
The diagnosis rests above all on a detailed history and a rigorous clinical examination.
The story of the pain provides essential information:
- initial location;
- mode of onset;
- aggravating or relieving factors;
- the possible presence of neurological symptoms;
- evolution over time.
The clinical examination then makes it possible to assess:
- lumbar mobility;
- muscular strength;
- sensation;
- reflexes;
- reproduction of the symptoms during specific tests.
The aim is to determine whether the pain is compatible with radicular involvement, referred pain, or involvement of the deep structures of the gluteal region.
Medical imaging is not routine. It is generally reserved for situations where symptoms persist, where a neurological deficit is present, or where a condition requiring specific treatment is suspected.
Key points
Sciatica is a symptom, not a disease. While a disc herniation with irritation of a nerve root is the most common cause, other conditions can produce very similar pain.
A rigorous clinical examination generally makes it possible to distinguish true radicular pain from its main differential diagnoses and to direct management appropriately.
When pain runs down the leg, the point is therefore not only to make the diagnosis of "sciatica," but above all to identify its cause precisely.
Further reading
If the pain is part of back trouble that lingers, our page on chronic low back pain offers further insight. Once the cause has been identified and outside any warning-sign situation, back stretches and back strengthening exercises may contribute to management.
Frequently asked questions (FAQ)
Is sciatica always caused by a herniated disc?
No. Lumbar disc herniation is the most frequent cause of true sciatica (involvement of a nerve root, most often L5 or S1), but many other mechanisms can produce pain radiating into the leg: deep gluteal syndrome, referred pain from the lumbar facet or sacroiliac joints, lumbar canal stenosis. Clinical examination distinguishes these situations.
What is "false sciatica"?
It is pain that mimics sciatica without true compression of a nerve root. The main causes are deep gluteal syndrome (formerly called piriformis syndrome), referred pain from the lumbar spine or pelvis (facet joints, discs, sacroiliac joint) and certain muscular tensions of the lumbopelvic region. Symptoms are similar but the clinical picture differs.
What warning signs require a rapid consultation?
Difficulty passing urine or controlling the bowels, loss of sensation in the genital or perineal region, significant or rapidly worsening muscular weakness, pain associated with fever, pain after a major injury, or severe persistent pain particularly at night. These signs may suggest cauda equina syndrome and require urgent care.
Is an MRI needed to diagnose sciatica?
No, not routinely. Diagnosis relies above all on the patient history and clinical examination (lumbar mobility, strength, sensation, reflexes, specific tests). Imaging is reserved for persistent symptoms, the presence of a neurological deficit, or when a specific condition requiring particular treatment is suspected.
References
- Jensen RK, Kongsted A, Kjaer P, Koes B. Diagnosis and treatment of sciatica. BMJ. 2019;367:l6273. doi.org/10.1136/bmj.l6273
- Ropper AH, Zafonte RD. Sciatica. N Engl J Med. 2015;372(13):1240-1248. doi.org/10.1056/NEJMra1410151
- Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ. 2007;334(7607):1313-1317. doi.org/10.1136/bmj.39223.428495.BE
- Stynes S, Konstantinou K, Dunn KM. Classification of patients with low back-related leg pain: a systematic review. BMC Musculoskelet Disord. 2016;17:226. doi.org/10.1186/s12891-016-1074-z
- Boyajian-O'Neill LA, McClain RL, Coleman MK, Thomas PP. Diagnosis and management of piriformis syndrome: an osteopathic approach. J Am Osteopath Assoc. 2008;108(11):657-664. doi.org/10.7556/jaoa.2008.108.11.657
- Hu YE, Ho GWK, Tortland PD. Deep Gluteal Syndrome: A Pain in the Buttock. Curr Sports Med Rep. 2021;20(6):279-285. doi.org/10.1249/JSR.0000000000000848
- Babu JM, Patel SA, Palumbo MA, Daniels AH. Spinal Emergencies in Primary Care Practice. Am J Med. 2019;132(3):300-306. doi.org/10.1016/j.amjmed.2018.09.022
This article offers general information and does not replace a personalised consultation with a healthcare professional.